
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 284-286
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 284-286
Letter To Editor
Death following Ventricular cerebrospinal fluid shunting in supratentorial malignant tumor associated with hydrocephalus
Muzumdar DP, Bhatjiwale MG, Goel A
Department of Neurosurgery, King Edward VII Memorial Hospital and Seth G. S. Medical College, Parel, Mumbai
Correspondence Address:Department of Neurosurgery, King Edward VII Memorial Hospital and Seth G. S. Medical College, Parel, Mumbai
dmuzumdar@hotmail.com
Code Number: ni04101
Sir
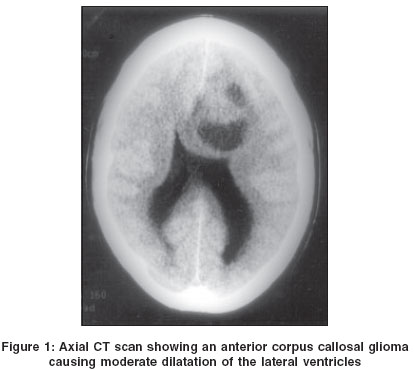
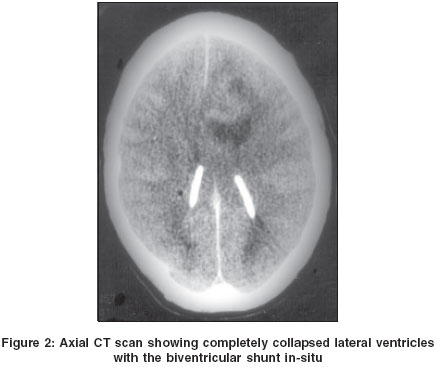
A 26-year-old male presented (in 1996) with complaints of headaches and right focal motor seizures for two years. The patient was dull and drowsy but had no higher function disturbance or focal neurological deficit. There was bilateral florid papilledema. Computerized tomography (CT) scan showed a large, anterior corpus callosal tumor and moderate hydrocephalus [Figure - 1]. A biventriculoperitoneal shunt was performed. The cerebrospinal fluid pressure was high and it flowed out like a ′jet′ through the cannula used during the shunt. Following surgery, the patient could not be reversed from anesthesia. Neurological examination three hours after surgery revealed that the patient was deeply unconscious and the left pupil was dilated and fixed. Within an hour, the right pupil also dilated and was unresponsive to light. Cerebral decongestants proved to be of no benefit. CT scan showed that both the ventricular catheters were in-situ and the ventricles were collapsed [Figure - 2]. The cerebral hemispheres showed extensive edema. The patient succumbed on the third postoperative day. Post-mortem examination showed swollen cerebral hemispheres and generalized cerebral edema.
Discussion Supratentorial intra-axial tumors lead to a rise in the intracranial pressure by virtue of the tumor mass and its surrounding edema. Occasionally, there is a ventricular dilatation as a result of direct or indirect compression of the cerebrospinal fluid pathways[1],[2]. In large hemispheric tumors, which result in a significant rise in the intracranial pressure, contralateral ventricular enlargement is frequently seen. Ventricular dilatation and cerebral edema are often considered to be a part of the pathological process. In our case an unconventional treatment strategy was adopted. A biventricular shunt was done. The aim of such a procedure was to attempt to reduce the intracranial pressure, relieve the patient of his symptoms, to normalize the altered cerebral blood flow and to ′relax′ the brain that would assist the surgeon in the definitive surgical procedure planned through an interhemispheric approach at a later date. The strategy was unsuccessful and the patient worsened dramatically after the shunt.
We attempted to analyze the cause of the fatal outcome in an otherwise well preserved patient and reviewed the relevant literature. As the shunt surgery in itself was uneventful and the postoperative scan did not show any evidence of hemorrhage, direct trauma by the shunt assembly appeared unlikely. It is known that ventricular tapping and shunt insertion in the presence of a large posterior fossa tumor may result in upward or reverse herniation or may result in subtle movements in the tumor due to a change in the naturally adjusted pressure dynamics following drainage of cerebrospinal fluid from lateral ventricles.[3],[4],[5]
Such movements may be the cause of hemorrhage in some tumors.[4],[6] Spinal tumor movement and impaction in the spinal canal and neurological worsening following a lateral ventricular shunt surgery has been recorded.[7] Posterior fossa, suprasellar and thalamic tumor patients have been recorded to worsen neurologically following a shunt operation.[3],[8] Tumor movement and alteration of the delicately balanced intracranial pressure have been implicated as the cause of the clinical worsening.[8],[9]
Our patient had a large tumor mass. The intraventricular pressure was high as was observed during the ventricular tapping whilst performing the shunt surgery. Both these factors contributed to a significantly high intracranial pressure. The neurological worsening following the ventricular tapping in our case suggests that the rise in the intraventricular pressure was in some manner maintaining or balancing the intracranial dynamics. Following the ventricular cannulation and rapid drainage of the cerebrospinal fluid, there could have been movements within the tumor or of the tumor as a whole. The large tumor could have probably impacted on to the hypothalamus or the internal capsule, or could have resulted in a subtle but definitive midline shift that initiated a chain of events that resulted in increased cerebral edema and later transtentorial herniation. There was no obvious hypoxic event during the induction of the anesthesia. Despite the fact that the cause of worsening in our case could not be actually confirmed, it appears that any form of ventricular drainage prior to surgery on large cerebral tumors associated with hydrocephalus is detrimental and should be avoided. The role of ventricular dilatation and the impact of a rise in the intraventricular cerebrospinal fluid pressure in the presence of a large intracranial tumor need to be evaluated further.
References
| 1. | Thapar K, Rutka J, Laws ER. Brain oedema increased intracranial pressure, vascular effects and other epiphenomenon of human brain tumour In: Kaye NH, Laws ER, (Ed). Brain Tumours. Edinburgh: Churchill Livingstone 1995:163-90. Back to cited text no. 1 |
| 2. | Ammirati M, Sami M, Sephernia A. Surgery of large retrochiasmatic craniopharyngiomas in childhood. Childs Nerv Syst 1990;6:13-7. Back to cited text no. 2 |
| 3. | Goel A. Whither preoperative shunts for posterior fossa tumours? Br J Neurosurg 1993;7:395-9. Back to cited text no. 3 [PUBMED] |
| 4. | Epstein F, Rajgopalan M. Paediatric posterior fossa tumours: Hazards of `preoperative' shunt. Neurosurgery 1978;3:348-50. Back to cited text no. 4 |
| 5. | Raimomdi AJ, Tomita T. Hydrocephalus and infratentorial tumours-incidence, clinical picture and treatment. J Neurosurg 1981;55:174-82. Back to cited text no. 5 |
| 6. | Vaquero J, Cabezudo JM, DeSola RG, Nombela L. Intratumoural haemorrhage in posterior fossa tumour after ventricular drainage. Report of two cases. J Neurosurg 1981;54:406-8. Back to cited text no. 6 |
| 7. | Koshu K, Tominaga T, Fujii Y, Yoshimoto T. Quadriparesis after a shunting procedure in a case of cervical neurinoma associated with hydrocephalus: Case report. Neurosurgery 1993;32:669-70. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Goel A. Preoperative shunts in suprasellar tumours. Br J Neurosurg 1995;9:189-93. Back to cited text no. 8 [PUBMED] |
| 9. | Goel A, Nitta J, Kobayashi S. Tumour-obstructive hydrocephalus: A natural defense mechanism In: Neurosurgery of Complex Tumours and Vascular Lesions, Kobayashi S, Goel A, Hongo K, (Ed). New York: Churchill Livingstone 1997:373-91. Back to cited text no. 9 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04101f2.jpg]
[ni04101f1.jpg]
|

{kind=link}
{kind=link}