 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 3, July-September, 2004, pp. 325-331 Original Article The treatment of complex dural arteriovenous fistulae through cranial base techniques Kattner KeithA, Roth ToniC, Nardone EmilioM, Giannotta StevenL Central Illinois Neuroscience Foundation, Bloomington, Illinois; Keck School of Medicine, University of Southern California, Los Angeles, California
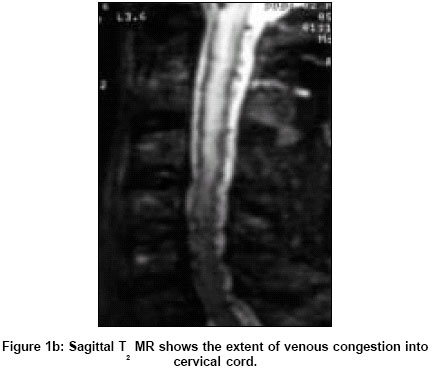
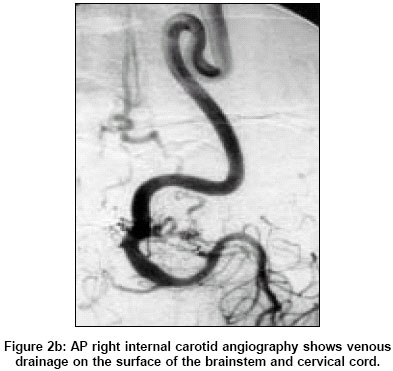
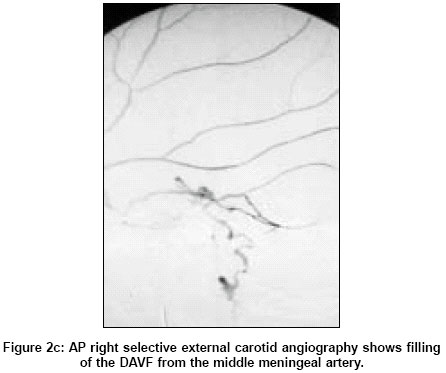
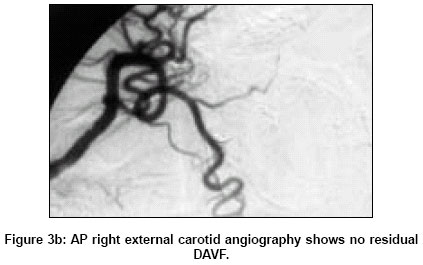
Correspondence Address:Central Illinois Neuroscience Foundation, 1015 South Mercer Avenue, Bloomington, Illinois - 61701 Code Number: ni04109 ABSTRACT Introduction: The endovascular modality of treatment is the preferred treatment modality for DAVF. In some circumstances, successful obliteration may not be possible by endovascular means, and such cases may require a direct surgical treatment. The authors report on their experience with the use of cranial base approaches in the treatment of deep and complex DAVF. Materials and Methods: Nine patients were treated between 1992 and 2003. There were six females and three males. Four patients presented with intracerebral hemorrhage, two with progressive myelopathy, two with tinnitus, and one with incapacitating chronic seizures. Four DAVF were tentorial, two transverse sigmoid, one craniocervical, one straight sinus, and one sphenoparietal. Endovascular embolization was attempted and unsuccessful in four cases, and was successful only as an adjunct to surgery in four others. All patients required the use of cranial base approaches to disconnect the fistula or resect the nidus. Results: Complete obliteration of the fistula was possible in all cases. Six-month follow-up results were obtained on seven patients where there was no evidence of recurrence. One postoperative temporal-lobe hematoma required surgical evacuation. One patient died two years postoperatively from an unrelated cause. Conclusion: This retrospective study demonstrates that complex DAVF can be successfully treated with the assistance of cranial base techniques. KEY WORDS: Arteriovenous fistula, dural, skull base Introduction Dural arteriovenous fistulae (DAVF) have the nidus of arteriovenous shunting within the dura mater.[1] They account for 10-15% of intracranial arteriovenous shunts.[2],[3] Blood supply comes from dural vessels and/or pachymeningeal branches of cerebral arteries. The vascular drainage of the fistulae occurs through either a venous sinus or leptomeningeal veins. The natural history of the DAVF is dependent on its venous drainage pattern.[1],[4] Intracranial DAVF that drain antegrade into a major dural sinus usually have a benign clinical course.[1],[5],[6],[7] However, if sinus drainage occurs with retrograde flow into arterialized leptomeningeal veins, or if the fistula drains solely into cortical leptomeningeal veins, a more aggressive natural history is seen.[1],[8],[9],[10],[11] Awad et al observed that patients with leptomeningeal venous drainage were 20 times more likely to suffer from progressive neurological deterioration or hemorrhage.[1],[9] Therapeutic options to treat DAVF include transarterial and/or transvenous embolization, surgical excision of the dural nidus, ligation of the draining vein, and stereotactic radiosurgery.[1],[7],[8],[9],[10],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24] The goal of treatment is complete and permanent obliteration of the fistula. The choice of treatment depends on the clinical presentation, anatomical location, arterial supply, and venous drainage pattern. Advances in endovascular techniques allow for a successful obliteration in a majority of these lesions. However, in some instances endovascular obliteration is not possible and surgical intervention is required. Standard craniotomy can be used to treat most superficial and simple DAVF. Deep-seated or complex DAVF require skull base techniques to provide the necessary exposure of the involved sinus. In the current study, the authors report on their experience with the use of cranial base approaches in the treatment of these difficult DAVF. Materials and Methods The clinical findings, angiographic characteristics, and surgical outcomes of nine patients treated through cranial base techniques were retrospectively reviewed. (Four patients have been previously reported.)[10] All nine patients presented to the neurosurgical service between 1992 and 2003 [Table - 1]. Presenting Symptoms All nine patients underwent six-vessel cerebral angiography. Four tentorial, two transverse/sigmoid, one craniocervical, one straight sinus, and one sphenoparietal DAVF were identified. Both transverse/sigmoid fistulae had antegrade flow with no retrograde or leptomeningeal drainage. The vein of Labbé had antegrade flow in both cases. All other DAVF had either pure leptomeningeal drainage or retrograde reflux from the involved sinus. Treatment Four cases of tentorial DAVF were treated employing an anterior petrosectomy approach. Three cases had feeding vessels from both the MPHA and the MMA. One patient also had feeding vessels from the AICA. Three cases were noted to have isolated SPS. Patient #2 was initially noted to have feeding vessels from the right MMA and MHPA. Drainage was leptomeningeal into the vein of Rosenthal. The SPS was isolated. The external circulation was embolized with PVA 150-250 microns and fibered microcoils. No transarterial embolization of the MHPA was attempted. Surgery was performed through a right frontal-temporal craniotomy. Extensive removal of the temporal fossa floor was required. Exposure of the V3 division of the trigeminal nerve in the foramen ovale was necessary. Transosseous feeding arteries were obliterated with a diamond drill. The MMA was coagulated and cut at the level of the foramen spinosum. This allowed extradural elevation of the temporal lobe. The greater superficial petrosal nerve (GSPN) was cut to avoid facial nerve damage from retraction. Removal of the bone posterior to the trigeminal nerve in Glasscock′s triangle exposed the petrous portion of the carotid artery. The bone in the Kawase′s triangle, posterior to the carotid artery, was removed up to the SPS. The dural sheath of Meckel′s cave was opened to expose the trigeminal nerve. The dura was then opened in a linear fashion from the inferior lateral temporal lobe to the SPS. Feeding arteries arising from the cavernous sinus were coagulated and cut. Once the SPS was encountered, it was clipped and cut, exposing the posterior fossa. The drainage vein was then identified and cut. The cranial base procedures for Patients 3 and 4 were performed in the same fashion. Patient #3 had draining directly into the petrosal vein. After the SPS was cut, the petrosal vein was coagulated and cut. Patient #4 had direct drainage into the SPS with reflux into superficial temporal veins. In this case, the entire medial half of the SPS was removed. Patient #5, who also had a tentorial DAVF with an isolated SPS, required an orbitozygomatic osteotomy. After the sectioning of the SPS, the draining veins were identified in the posterior fossa. They were then coagulated and cut. Two cases had transverse sigmoid sinus fistula. Patient #6 had multiple feeding vessels, including the left OA, VA, MMA, MHPA, and AMA. N-butyl cyanoacrylate (NBCA) embolization was used to treat the OA, MMA, and AMA. Tinnitus resolved following treatment; however, her symptoms of tinnitus returned 6 months later. The patient refused further endovascular treatment. Surgery was then offered as an option for the patient. Extensive removal of bone was necessary to skeletonize the TSS. This was accomplished through combined retrosigmoid and retrolabyrinthine bony removal. The jugular bulb was exposed by transcondylar removal of bone, including the jugular tubercle. Complete removal of the TSS from the vein of Labbé to the jugular bulb was achieved. Five mm of the lateral SPS was also removed with the TSS. Patient #7 also presented with a TSS-DAVF. Multiple ipsilateral feeding vessels were noted on the left MHPA, MMA, AMA, STA, OA, PICA, PMA, and VMA. Antegrade flow was also noted from the vein of Labbé. Embolization of the TSS was not attempted. This could not be performed safely because of the proximity of the feeding vessels to the antegrade draining vein of Labbé. Bone removal also was used to skeletonize the TSS. This included a large retromastoid craniotomy with a combined petrosectomy. Jugular bulb exposure was not required in this case; therefore, a transcondylar approach was not necessary. The sinus was resected from the vein of Labbé to the lower portion of the sigmoid sinus. The SPS was also cut in the medial portion. One case of an isolated straight sinus was treated. Multiple right meningeal feeding vessels arose from the VMA on the right side. They traveled through the dura onto the roof of the tentorium towards the straight sinus. Instead of draining into the straight sinus, a large vein drained the fistula onto the superior surface of the right cerebellar hemisphere. Right VMA embolization with PVA was attempted but was unsuccessful. A right combined suboccipital and transcondylar craniotomy was performed. Transcondylar removal of bone allowed access to the origin of the multiple VMA feeders. The VMA was cut at its origin from the VA. This reduced hemorrhage during exposure of the draining vein. The draining vein was accessed through inferior retraction of the right cerebellar hemisphere. The vein was coagulated and cut where it bridged from the tentorium to the superior surface of the cerebellum. Patient #9 presented with a rare sphenoparietal DAVF. A single feeding vessel arose from the ophthalmic artery and drained directly into the sphenoparietal sinus. Retrograde flow occurred into the temporal bridging veins. Attempted arterial embolization was unsuccessful. The feeding artery could not be safely cannulated. The fistula was surgically approached via a standard pterional craniotomy. The sphenoid bone was removed, exposing the artery as it entered the sphenoparietal sinus. This vessel was coagulated and cut as it entered the sinus. The sphenoparietal sinus was not resected. Surgical procedures and outcomes are summarized in [Table - 2]. Results Immediate postoperative angiography revealed complete obliteration of all DAVF. Seven patients underwent follow-up angiography at six months. There was no evidence of recurrence in any of these cases. All presenting symptoms not related to presenting hemorrhage resolved after surgical obliteration. The two patients with transverse/sigmoid fistulae had complete resolution of their tinnitus after resection of the sigmoid sinus. No seizures have been reported in the one patient who presented with intractable chronic epilepsy secondary to a tentorial dural fistula. The two patients presenting with rapidly progressive brainstem dysfunction from venous hypertension had complete reversal of their symptoms after surgery. One patient had immediate improvement of her myelopathy. One patient with a tentorial dural fistula developed a temporal lobe hematoma. The temporal lobe hematoma was evacuated without consequence. One patient died two years after surgery from an unrelated glioblastoma. One patient had a slight ataxia, and another patient has persistent seizure activity. Both of these were probably a result of presenting intracranial hemorrhage. Case presentation: Patient #5: DISCUSSION Dural arteriovenous fistulae have a variable natural history that ranges from benign to aggressively life-threatening. This is related to the type of venous drainage. Awad et al[1] observed that a DAVF with leptomeningeal drainage had a much more aggressive natural course. Patients with this drainage pattern were 20 times more likely to have progressive neurologi cal deterioration.[1],[9] Borden et al defined the venous drainage pattern into three groups.[4] Type I fistulae involve antegrade drainage into a major draining sinus. In these cases no venous hypertension occurs and the clinical course is benign. Type II fistulae drain into a major sinus but create a retrograde flow into other veins that also drain into the same sinus. In these cases neurological deterioration and hemorrhage results from the venous retrograde hypertension occurring within these veins. Type III fistulae do not have any communication with a sinus and drain only into the leptomeningeal vein. Many Type III DAVF are in close anatomical proximity to a large draining sinus but do not communicate with it. The goal of treatment should be complete and permanent elimination of the arteriovenous shunt. Several options are available for the treatment of DAVF, including arterial embolization, transvenous occlusion, stereotactic radiosurgery, and direct surgical obliteration.[1],[7],[8],[9],[10],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24] Endovascular Treatment Transarterial embolization has been suggested as an initial treatment. Tomak et al[21] presented their series of 22 patients with tentorial DAVF. Eleven patients were treated between 1996 and 2000 with transarterial embolization. Five patients were cured. However, only one patient underwent an angiogram after six months; therefore, long-term recurrence cannot be assessed. Successful complete obliteration of a fistula through arterial access is less than 50%.[12] In cases with small diameter internal circulation feeding vessels, there is also an increased risk of stroke.[4],[15],[16],[18],[23] Stereotactic Radiosurgery Radiosurgery represents an important adjunct to the treatment of DAVF. However, it should be reserved for benign DAVF that have failed other treatments. Aggressive DAVF require urgent and complete obliteration that cannot be provided by radiosurgery.[9],[21],[23] Surgical Treatment Cranial base techniques have only recently been described in treating DAVFs.[10],[13],[18] Lewis et al[18] described four patients who were treated through cranial base techniques. Three tentorial and one inferior petrosal DAVF were treated through either anterior, posterior, or combined petrosectomy. De Jesús[13] utilized an anterior petrosectomy to treat a tentorial DAVF. This approach allows access to both the temporal and posterior fossa. Multiple transosseous feeding arteries are treated by using a diamond drill. If the craniotomy is supplemented with an orbitozygomatic osteotomy, less temporal lobe retraction is required. Resection of the sinus may not be necessary and the fistula can be treated by disconnecting the draining vein. However, if the sinus must be resected or posterior fossa access is necessary, the removal of the petrous apex allows 360° exposure of the petrosal sinus. Dural arteriovenous fistulae that occur at the craniocervical junction can be exposed through transcondylar bone removal. Access to the vertebral artery as it penetrates the dura is necessary to expose a fistula in this location. The authors utilized this approach in a straight sinus fistula to reduce bleeding before the suboccipital craniotomy was performed. Disconnection of the sphenoparietal fistula required exposure by extensive removal of the lesser sphenoid wing. The resection of the extradural bone to the meningo-orbital band exposed the abnormal vessel. This was an example of disconnecting a fistula extradurally, which could not have been accomplished through an intradural exposure. Transverse/sigmoid fistulae are exposed through skeletalization of the transverse-sigmoid junction. The proximal exposure of the superior petrosal sinus can be achieved through a partial posterior petrosectomy. The craniotomy can be extended down to the jugular bulb by transcondylar removal of bone. The entire sigmoid sinus can be resected if necessary. Most transverse/sigmoid fistulae are successfully treated through transvenous coil embolization. In some cases, surgical exposure of the sinus is required because the sinus is either isolated or obstructed. [25],[27],[28] Endo et al[28] successfully obliterated eight cases of TSS-fistulae through direct packing of the isolated sinus. Houdart et al[25] also had successful obliteration of five cases of TSS-fistulae utilizing direct packing through a small craniectomy. However, even in completely obliterated TSS-fistulae, direct packing is not always successful. Goto et al[27] reported that surgical resection of the TSS was necessary in 4 of 17 cases treated with direct packing. Based on these reports, it is relevant to include sinus resection as a form of treatment. CONCLUSION Dural arteriovenous fistulae have a variable clinical history. Most DAVF can be treated successfully by endovascular techniques. However, in some circumstances this may not be the optimal treatment for complete and permanent obliteration. Standard surgical techniques may not be successful in gaining good exposure to the arteriovenous fistula or nidus. By utilizing cranial base techniques, DAVF can be successfully treated with minimal morbidity and mortality. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04109f2c.jpg] [ni04109f3a.jpg] [ni04109f2a.jpg] [ni04109f3b.jpg] [ni04109f1a.jpg] [ni04109t1.jpg] [ni04109t2.jpg] [ni04109f1b.jpg] [ni04109f2b.jpg] |
| |||||||||

![[Table - 1]](/showimage?ni/photo/ni04109t1.jpg){kind=link}
![[Table - 2]](/showimage?ni/photo/ni04109t2.jpg){kind=link}
![[Figure - 1] a](/showimage?ni/photo/ni04109f1a.jpg){kind=link}
{kind=link}
![[Figure - 2]a](/showimage?ni/photo/ni04109f2a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 3] a](/showimage?ni/photo/ni04109f3a.jpg){kind=link}
{kind=link}