 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
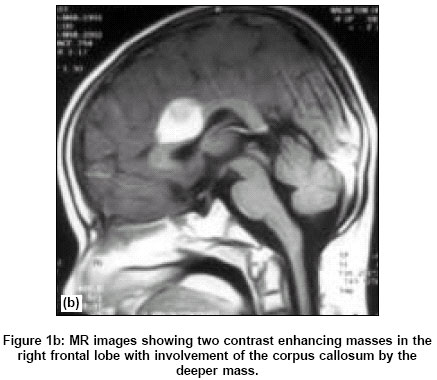
Neurology India, Vol. 52, No. 3, July-September, 2004, pp. 375-377 Case Report Glioblastoma multiforme in a child with acute lymphoblastic leukemia: Case report and review of literature Shah KiritC, Rajshekhar Vedantam Department of Neurological Sciences, Christian Medical College Hospital, Vellore Code Number: ni04121 ABSTRACT An 11-year-old boy with acute lymphoblastic leukemia had received prophylactic cranial irradiation (1800 cGy /10 fractions) and intrathecal methotrexate. Five years later, he developed a glioblastoma multiforme in the right frontal region while the leukemia was in remission. It is possible that the glioma may have been induced by radiation and /or chemotherapy.KEY WORDS: Brain tumor, radiation therapy, acute lymphoblastic leukemia INTRODUCTION Induction of neoplasia after therapeutic irradiation is well recognised.[1],[2],[3] Neoplasia of the central nervous system after radiation therapy has been documented in the form of meningioma and sarcoma. The occurrence of the glial tumor has been documented less frequently in association with radiotherapy. With the advent of effective combination chemotherapy, children with acute lymphoblastic leukemia (ALL) were noted to experience prolonged hematologic remission. However, the remission was interrupted in up to 65% of patients by the emergence of the central nervous system (CNS) leukemia, which frequently heralded subsequent systemic relapse. Intrathecal methotrexate either alone or in combination with cranial or craniospinal irradiation is effective in preventing initial CNS relapse in most patients. Although the long term sequelae of CNS prophylaxis have been well documented as leucoencephalopathy, neuropsychologic and intellectual impairment,[4],[5] the occurrence of glioblastoma multiforme has been documented less frequently in association with prophylactic irradiation and chemotherapy. Well-accepted criteria have been established to show causal relationship between radiotherapy and occurrence of a subsequent neoplasm. These include: a prolonged delay between irradiation and the detection of second tumor, that the second tumor be in the irradiated field, that the histological type of the second tumor be of a different cell line than the initial neoplasm and that the incidence of the second lesion is significantly higher than in controls. This case report describes a patient who developed a cerebral glioblastoma five years after prophylactic cranial irradiation and chemotherapy for ALL. CASE REPORT An 11-year-old boy was diagnosed to have ALL in April 1997. He was treated with induction chemotherapy (prednisolone, vincristine, doxorubicin and L-asparaginase) and had received 12 doses of intrathecal methotrexate during that period. From June 26 to July 10, 1997 Cobalt irradiation was given to the whole brain with a daily dose of 180 cGy. A total dose of 1800 cGy was delivered in 10 fractions over 14 days. Maintenance therapy was methotrexate at weekly intervals. He continued to receive methotrexate at weekly intervals, till June 1999. At that time all medications were stopped after proving complete remission by bone marrow examination. He never had a relapse and continued to be in remission. He was admitted to our hospital in March 2002 with two episodes of left focal motor seizures, 15 days prior to admission. Physical examination was normal. Laboratory findings revealed a hemoglobin 12 gm/dl, total leukocyte count 4000/cmm and platelet count of 1,44000/cmm. CT scan and MRI of the brain showed two right frontal mass lesions [Figure- 1]a-b. He underwent CT guided stereotactic craniotomy and partial excision of the superficial lesion . Histologically, the tumor was a highly cellular, anaplastic glial neoplasm with areas of necrosis and endothelial proliferation. There was prominent mitotic activity. On immunohistochemistry, the tumor was positive for glial fibrillary acidic protein (GFAP) and negative for L26, CD3 and CD43. On the basis of these findings, a diagnosis of glioblastoma multiforme was made. Post-operatively the patient was treated with cranial irradiation . A dose of 4500 cGy was given to the whole brain. DISCUSSION The apparent induction of a second malignant neoplasm by antineoplastic therapy is no longer a surprising observation. Though it is impossible to prove, the glioblastoma in our patient was most likely treatment induced, whether by radiation, chemotherapy or both. It may have been "spontaneous" although this is unlikely considering the low incidence of glioblastoma of the cerebrum in children. The other possibility is a biologic predisposition to neural crest and neuroectodermal tumors as is seen in Von Recklinghausen′s disease. The negative family history and the lack of peripheral manifestation of Von Recklinghausen′s disease suggests that it was not a factor in the present case. Radiation induced brain tumors are well known. Modan et al[6] followed 11,000 children irradiated for ringworm of the scalp and two matched control groups. Results of that study indicated that there was a significantly increased risk of head and neck tumor following radiation. Most radiation associated intracranial neoplasms have been sarcomas or meningiomas.[7],[8],[9]Only few cases of radiation induced glioblastoma in humans have been reported.[10],[11],[12] The radiation dose ranged from 400-6000 cGy with latent period of an average of nine (1-29) years. The first fully documented case of CNS glioma following prophylactic treatment of ALL was reported in 1979.[13] Study of large number of patients (1,612) with ALL showed the cumulative incidence of brain tumor at 20 years is 1.39%.[14] [Table - 1] shows fully documented cases of CNS glioma following CNS prophylactic treatment for ALL.[15],[16],[17],[18],[19] There were a total 14 cases out of which 5 had glioblastomas. The age of the patient at the presentation of brain tumor ranged from 2 years to 19 years. The glioblastoma was commonly located in the frontal region. The dose of prophylactic cranial radiation received by the ALL patients ranged from 1800 to 2623 cGy. The interval from radiation therapy to occurrence of the brain tumor ranged from 48 months to 11 years. Although the role of radiation in carcinogenesis had been well established in humans and experimental animals, the exact mechanism of radiation induced carcinogenesis remains to be elucidated. It was demonstrated that radiation induced neoplasm appears to arise through mutagenic capacity and chromosome aberration and the mechanisms leading to neoplastic transformation involves multistage processes (multi-hit kinetics) rather than a single, one-hit type of biochemical alteration. The other possible etiologic factor in induction of our patient′s tumor could be the combination of intrathecal methotrexate with cranial irradiation.[20] It is known that administration of methotrexate in combination with 200 cGy or more cranial irradiation may result in multiple necrotic areas with or without gliosis disseminated throughout the cerebral white matter (leukoencephalopathy).[21] However, there is no evidence in man or experimental animal to indicate that intrathecal methotrexate alone is carcinogenic or that it enhances the carcinogenic effect of radiation. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04121t1.jpg] [ni04121f1a.jpg] [ni04121f1b.jpg] |
| |||||||||

![[Figure- 1]a](/showimage?ni/photo/ni04121f1a.jpg){kind=link}
{kind=link}
![[Table - 1]](/showimage?ni/photo/ni04121t1.jpg){kind=link}