 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
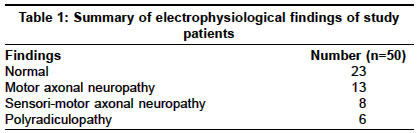
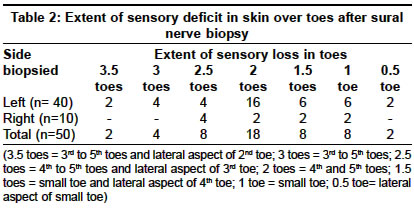
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 436-438 Original Article Variability in the extent of sensory deficit after sural nerve biopsy Kumar Sudhir, Jacob J Neurology Unit, Department of Neurological Sciences, Christian Medical College, Vellore - 632 004 Code Number: ni04149 ABSTRACT BACKGROUND: Sural nerve biopsy (SNBx) is associated with multiple complications such as paresthesia, pain, or numbness in the sural nerve distribution at the site of biopsy and wound infection. An accurate idea of these adverse events would be useful while taking informed consent from patients.AIMS: We conducted a prospective study to determine the extent of sensory deficits after SNBx. SETTINGS AND DESIGN: It is a prospective, hospital-based (tertiary teaching hospital) study. MATERIALS AND METHODS: All the patients who had SNBx between May 2003 and March 2004 were eligible for inclusion. However, patients with sensory impairment in sural nerve territory or abnormal sural nerve conduction studies prior to the procedure were excluded. SNBx was performed in the ankle region under local anesthesia, and a 3 cm nerve segment was excised. Touch, pain, temperature, vibration and joint position were tested after the nerve biopsy. The extent of sensory deficit was determined. Any other complications, when present were also noted. Follow-up assessment was performed at three months or later. RESULTS: Fifty patients (26 women) fulfilled the inclusion and exclusion criteria. The mean age was 37.4 (16-63) years. One-two weeks after the SNBx, 46 (92%) patients had sensory deficit along the lateral aspect of the foot at the site of the biopsy, and 48 (96%) patients had sensory impairment extending beyond the outer aspect of the fifth toe. At follow-up, sensory deficit was present in 89% patients and paresthesia in 39%. CONCLUSIONS: The majority of the patients undergoing SNBx develop persistent sensory deficits, which often extend beyond the typical sural nerve territory. Key Words: Sural nerve biopsy, Complications, Sensory deficit, Variations INTRODUCTION Sural nerve biopsy (SNBx) is one of the most common procedures employed in the evaluation of peripheral nerve disorders. It is particularly useful in establishing the diagnosis of certain neuropathies like leprosy, vasculitic neuropathy, amyloid neuropathy, sarcoid neuropathy, and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).[1] In about two-thirds of the patients the results of SNBx are likely to alter the management.[2] However, the procedure is associated with a number of complications such as persistent sensory loss, pain and paresthesia in the territory of the sural nerve, painful neuromas, and infection at the biopsy site.[2],[3],[4],[5],[6] The extent of sensory deficit (Sdef) following SNBx varies widely. Therefore, it is prudent to balance the diagnostic yield of SNBx against the complications, so that a better informed consent can be obtained from patients. MATERIALS AND METHODS This prospective study was conducted in the Neurology Department of a tertiary teaching hospital. All consecutive inpatients admitted between May 2003 and March 2004 who had an SNBx were eligible for inclusion. However, patients with evidence of Sdef prior to the procedure or with abnormal sural nerve amplitude were excluded. Informed consent was obtained from all the patients. Technique of SNBx: The sural nerve was exposed after making an incision midway between the lateral malleolus and tendoachilles. Whole sural nerve biopsy was performed and a 3 cm segment of the nerve was excised. Severed ends of the nerve were not sutured.[7] The procedure was done under local anesthesia. Sensory Assessment: Detailed sensory testing for touch, pain, temperature, vibration and joint-position was performed between the 7th and 14th days after the procedure. Touch was tested using a wisp of cotton, pain using a sharp pin, temperature using test tubes filled with hot or cold water, and vibration was tested with a 128-Hz tuning fork.[8] Sdef was considered to be present if there was absence or reduced perception of any of the modalities tested. Sensory assessment was also performed on the normal side (the non-biopsied side). The sensory assessment was repeated after three months or later. Even though the authors were part of the treating team, which decided to perform SNBx, they however had no direct influence on the decision. RESULTS A total of 50 patients (26 women) fulfilled the inclusion and exclusion criteria. The mean age was 37.4 years (16-63 years). Pre-biopsy diagnosis included vasculitis (36 patients), leprosy (10 patients), and CIDP (8 patients) (some patients had more than one indication). The duration of symptoms ranged from five days to seven years (mean 11 months). Findings obtained on nerve conduction studies are summarized in [Table - 1]. All the patients had normal sural nerve conductions and none had any sensory deficit in the territory of the sural nerve prior to the procedure. Biopsy was performed on the left side in 40 patients and on the right side in 10. Extent of Sdef: Sdef along the lateral aspect of the foot was present in 46 (92%) patients. Sdef over the dorsal aspect of the toes varied widely [Table - 2]. Forty-eight patients (96%) had Sdef extending beyond the outer aspect of the small toe. Other complications: Postoperative pain was present in 21(42%), and paresthesia in 18 (36%) patients. Infection at the biopsy site was noted in four (8%). Yield of nerve biopsy: SNBx yielded a definitive diagnosis in 17 (34%) patients [Table - 3]. Of the remaining 33 patients with normal findings on SNBx, the procedure was helpful in excluding vasculitis in 24 patients (final diagnosis in them included acute disseminated encephalomyelitis (ADEM) in 12, multiple cerebral infarcts in 10, isolated central nervous system angiitis and central nervous system lupus in one each) [Table - 3]. Thus, SNBx played an important role in the management of 41 (82%) patients. There was no correlation between the etiology or the extent of neuropathy and the complication rate. Follow-up: A total of 36 patients were seen at intervals ranging from 3-10 months (mean 6.3 months) after the procedure. Sdef was present in 32 (89%) and paresthesia in 14 (39%) patients. The wound had healed in two of these patients who initially had infection of the biopsy site. Fourteen (39%) patients had persistent pain in the sural nerve territory. None of the patients had any impairment in the activities of daily living or ever consulted a physician for these symptoms. DISCUSSION Sural nerve biopsy is an established procedure employed for evaluating peripheral neuropathy. Notwithstanding the usefulness of SNBx in the diagnostic evaluation and management of patients with peripheral neuropathy, this procedure is associated with several complications. These include persistent pain (67%),[2] dysesthesia, paresthesia, and sensory deficit in the sural nerve territory, neuroma formation at the severed end of the nerve and infection (10-15%)[2],[4] at the biopsy site. These symptoms may persist for many months; 33% out of 54 patients reported paresthesias and 19% had dysesthesias after a follow-up of 5-32 months.[9] Sensory deficit after SNBx is another major problem, as noted in 93% of the patients in two studies.[3],[9] The follow-up period in these two studies was 21 and 5-32 months respectively. In our study, 89% had sensory deficit at a mean follow-up period of six months; however, our patients demonstrated a great variability in the extent of Sdef. The most consistent area of Sdef was the lateral aspect of the foot, in 92% of patients. Sdef over the dorsal aspect of the toes was present in all, however, it ranged from only the outer aspect of the 5th toe to three and a half toes (3rd to 5th toes and outer aspect of the 2nd toe) [Table - 1]. The union of the medial and lateral sural cutaneous nerves forms the sural nerve. Though this union occurs at various sites, the commonest site is the lower third of the leg.[10] In the dorsum of the feet, communications may be noted between the branches of the dorsal sural nerve and the lateral branches of the distal superficial peroneal nerve. Typically, the superficial peroneal nerve is believed to supply the dorsal skin of all toes, except the lateral side of the 5th toe (supplied by the sural nerve) and the adjoining sides of the great and 2nd toes (supplied by the deep peroneal nerve).[11] However, in our series, 96% of the patients had Sdef extending beyond the typical distribution of the sural nerve (outer aspect of the 5th toe). Our study is probably the first prospective study that evaluated the variability in Sdef following SNBx. All the studies including the present study demonstrate a significant, often persistent Sdef after SNBx. Some studies studied the possible associated factors that may predispose the patients to develop sensory deficit following SNBx: (i) Diabetes Mellitus: In a prospective study, the extent of Sdef at 6, 12, or 18 months did not differ between patients with and without diabetes mellitus.[12] However, in another study, mild persistent sensory symptoms were significantly more common in patients with diabetes mellitus (64%) when compared to patients without diabetes mellitus (28%). The follow-up period was about six years.[13] These symptoms, however, did not interfere with the activities of daily living or warrant any medical therapy. In our series, only three patients had diabetes, and the Sdef was confined to the outer aspect of the 5th toe in two and to both sides of the 5th toe in one. (ii) Sural Nerve Action Potentials (SNAPs) prior to SNBx: It was reported that patients with detectable SNAPs were twice as likely to develop a new numbness as compared to those with absent SNAPs.[2] However, in another study, the diagnostic yield of SNBx increased in patients with a greater reduction in motor conduction velocities.[14] (iii) Length of the nerve excised: No correlation was observed between the length of the nerve excised and the complication rate.[4] (iv) Fascicular versus whole sural nerve biopsy: Pollock et al reported no significant difference in areas of sural sensory loss between fascicular and whole nerve biopsy groups.[15] The possible reasons include (1) cutting interfascicular branches during the 3-5 cm fascicular dissection may cause more extensive damage to the sural nerve than would be anticipated from the number of fascicles removed and (2) the blood supply to intact fascicles might be compromised by damage to the vasa nervorum. Whole nerve biopsy for sural nerve, therefore, is recommended as it is simpler, has greater diagnostic potential, and allows for a more complete morphological evaluation without increasing the complication rate. It is clear from the foregoing discussion that the Sdef after SNBx is inevitable and no factor seems to alter the extent or rate of this complication. Therefore, the current interest has shifted to post-biopsy care. Schoeller et al recently reported the benefits of microsurgical repair of the sural nerve after nerve biopsy.[16] This procedure involves careful mobilization of the proximal and distal nerve stumps after resecting a 10-mm segment of the sural nerve under local anesthesia, and uniting with epineural suture techniques, under a surgical microscope. A return of sensations in the sural nerve territory to the pre-biopsy level was noted as early as six months after the microsurgical repair. It should be mentioned here that this technique is in a preliminary stage and further studies are needed before a final recommendation can be made. Patients included in our study had normal sensations in the sural nerve territory and normal sural nerve conductions. This is quite different from the routine clinical situation, where most of the patients undergoing SNBx biopsy have significant neuropathy, clinically or electrophysiologically or both. In fact, during our study period, 81 such patients were excluded. Therefore, data obtained from this study cannot be generalized to all patients undergoing SNBx. In summary, SNBx leads to Sdef in the sural nerve territory in almost all the patients, which persists for many years. Our study has shown that the extent of Sdef is highly variable and 96% of patients have deficits beyond the region of the classical sural nerve distribution (outer aspect of the little toe). It is important to inform about the possibility of a more extensive Sdef to the patients prior to the SNBx to avoid dissatisfaction later. The encouraging fact for us, however, is that the post-biopsy complaints are mild and almost never interfere with the activities of daily living. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04149t1.jpg] [ni04149t2.jpg] [ni04149t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}