
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 4, 2004, pp. 439-442
|
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 439-442
Original Article
Intracranial cavernomas: Analysis of 37 cases and literature review
Kayali Hakan, Sait Sirin, Serdar Kahraman, Kaan Oysul, Ilker Solmaz, Erdener Timurkaynak
Departments of Neurosurgery, Oncology of Gulhane Military Medical Academy, Ankara
Correspondence Address:Department of Neurosurgery, Gulhane Military
Medical Academy, 06018, Etlik-Ankara, hakankayali@hotmail.com
Code Number: ni04150
ABSTRACT
AIMS: Thirty-seven patients with intracranial cavernomas managed in our department are retrospectively analyzed.
MATERIALS AND METHODS: The data of 37 patients with cavernoma who were admitted to our department between 1995 and 2003 were reviewed retrospectively. There were 30 male and 7 female patients with a median age of 26 years (range, 9-57 years). Four cases were treated surgically, 13 were treated by stereotactic radiosurgery (SRS) and the remainder were managed conservatively.
RESULTS: New hemorrhage or additional neurological deficits were not observed in the surgically treated cases, 12 patients who underwent SRS and the other patients who were followed up. One of the 13 patients treated by SRS, underwent microsurgery due to increased seizure frequency. One of the patients treated surgically died on the 11th postoperative day.
CONCLUSION: Clinical observation should be the choice of management for patients without new or progressive neurological deficits, without two or more hemorrhages and in patients where the seizures are controlled with drugs. Surgery is the first choice for the cavernomas located in the non-eloquent locations. Radiosurgery may be an alternative for patients having deep-seated and eloquent area located cavernomas and for patients not willing or suitable for surgery.
Key words:
INTRODUCTION
Cavernoma is a benign vascular hamartoma. Approximately 50% of the cases are multiple.[1] They rarely occur in the spinal cord.[2],[3] The onset of symptoms is usually in the third or fourth decade of life, although some cavernomas have presented in childhood.[4] Retrospective surgical series show good results after surgery, but the outcome in such patients if they had not undergone surgery is unknown.[5] Recently, radiosurgery has been proposed for the treatment of cavernomas located in an eloquent region of the brain.[6],[7],[8] We review our experience with 37 cases of cavernomas.
MATERIALS
AND METHODS
The data of 37 cavernoma cases (30 males, 7 females) admitted to our department between 1995 and 2003 were reviewed retrospectively. The median age was 26 years (range, 9-57 years). Clinical features are summarized in [Table
- 1] and [Table -
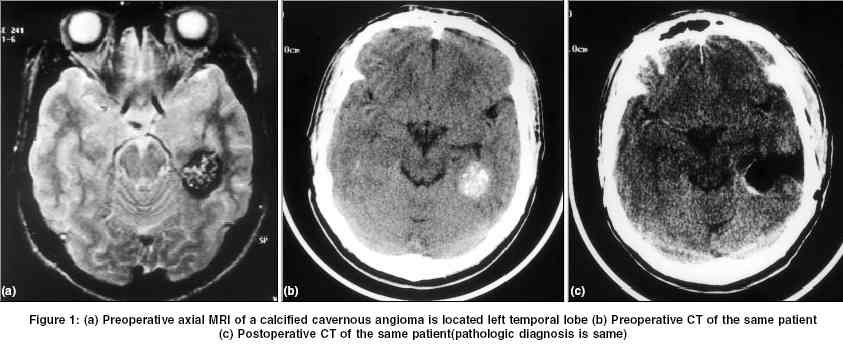
2]. In all the patients, computed tomography (CT) and magnetic resonance imaging (MRI) were performed. Locations of the lesions were 57% supratentorial. Electroencephalogram (EEG) was performed in 19 patients presenting with seizures. Except for two cases, the EEG was abnormal and concurrent with the site of the lesion. Digital substraction angiography (DSA) was performed in 5 patients who had hemorrhage. The angiogram did not reveal any vascular abnormality. Four cases were treated surgically [Figure
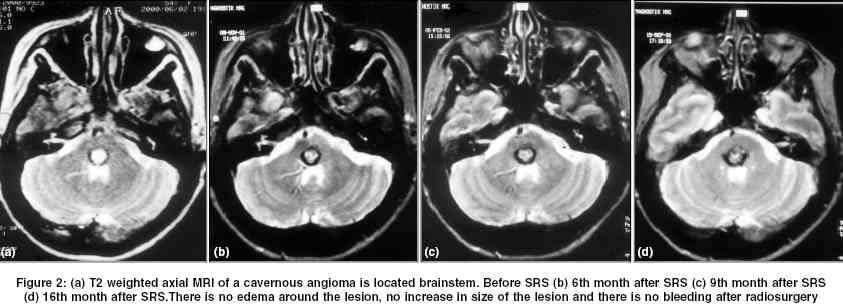
- 1], 12 cases were treated by SRS and the rest of the patients were managed conservatively. The criteria for the conservative management of cavernoma were when the seizures were controlled with antiepileptics, there was no progressive neurological deficit and when there were less than two hemorrhages. The patients′ preference was taken into consideration. Two patients with frontal cavernoma were treated by SRS as they did not accept the surgical treatment. In radiosurgical treatment, Linear Accelerator (Philips SL-25, UK), Isocentric subsystem (Philips K-X 200, UK), Brown-Roberts-Wells Head Frame (Radionics Co., USA) and X knife3 planning system (Radiosonics Software Applications Inc., USA) were used. 6 MeV X-ray was produced by Linear Accelerator. In all cases single isocenter, median 310 degree total arch angle (300-320) and median 6 arch (5-7) were used. Median 15 Gy (14-20) was applied to the peripheral zone of the lesion (80%) [Figure
- 2].
RESULTS
A 40-year-old female who also had multiple sclerosis and was treated surgically for brainstem cavernoma died on the 11th postoperative day. Of the 13 patients treated by SRS, one patient with frontal cavernoma (9-year-old patient whose surgical treatment was not accepted by his parents) had an increase in seizure frequency refractory to medical treatment and underwent surgery in the 12th month after radiosurgery. The median follow-up period was 2.5 years (1-8 years). None of the patients in the series had any neurological or radiological deterioration. DISCUSSION
The etiology of cavernomas is unknown. Cranial radiation, coexistent vascular malformation, genetic, and hormonal factors all have been implicated for the cavernomas. The proportion of patients developing clinical symptoms is higher in the hereditary form than in the sporadic form of the cavernoma.[9],[10],[11],[12],[13],[14],[15],[16] De novo formation of a cavernoma during immunosuppressive treatment has also been reported.[17] There are some radiation-induced cavernomas occurring in childhood and adolescence.[18] Cavernoma was reported in 0.39% of 8131 patients evaluated with craniospinal MRI.[19] Our incidence was 3%, with 37 patients with cavernous angioma out of 1228 patients with intracranial mass lesion treated during the period. The majority of the cavernomas are supratentorial in location.[19] In our series 43% of the lesions were located infratentorially. Approximately 60% patients present with seizures, 50% patients have progressive neurological deficit and 20% patients have hemorrhage in intracranial cavernomas.[20],[21] Despite the preponderance of cavernomas above the tentorium cerebelli, the general belief is that hemorrhage is more likely to occur from infratentorial lesions.[19],[21] The location of the lesion is an important factor in predicting hemorrhage or the neurological course. In another series all hemorrhages occurred in the cavernomas located supratentorially.[22] In our series hemorrhage was observed in 5 patients (13.5%). Three of the hemorrhages (60%) were supratentorial. MR features of cavernomas are characteristic and diagnostic of these lesions obviating the need for angiography.[23] Evidence of a recent or old hemorrhage is commonly present in cases of cavernomas, including hemosiderin-laden macrophages, cholesterol crystals and deposits of hemosiderin in the surrounding parenchyma.[24] We observed calcified cavernomas in two patients. Calcified cavernomas are called "hemangioma calcificans" or "brain stone".[25],[26],[27] Cavernomas have been located in a variety of cranial sites.[28],[29],[30],[31],[32],[33],[34],[35],[36],[37],[38] Pediatric cavernomas are still diagnostically and therapeutically challenging lesions. There is a higher risk of hemorrhage in children when compared to adults.[39] Although some authors have stated that there was no difference in the hemorrhage rate before and after radiosurgery,[6] other authors recommend it especially for the brainstem, deep and eloquent located cavernomas, and a significant reduction has been observed in the annual hemorrhage rate after radiosurgery.[40],[41],[42],[43],[44],[45],[46] X-knife radiosurgery was performed for 13 patients in our series and the results were uneventful except for one pediatric case. Hemorrhage, edema around the lesions and increase in the size of the lesions were not observed in our 13 patients treated radiosurgically up to date [Figure
- 2].
Although the dominant role of surgery in cavernomas is recently undergoing re-evaluation, an accessible causative cavernoma is an indication for surgical resection.[19]
CONCLUSION
Conservative treatment for cavernoma should be the choice for the patients without new or progressive neurological deficits and two or more documented hemorrhages and with seizure responsive to the medical treatment. For the others, the treatment is primarily surgical for the cases with non-eloquent locations and the results have been best where complete excision is achieved. Radiosurgery may be an alternative for treatment of deep and eloquent area located cavernomas and for the patients who do not accept surgical treatment.
REFERENCES
| 1. | Rigamonti D, Drayer BP, Johnson P. The MRI Appearance of Cavernous Malformations (Angiomas). J Neurosurg 1987;67:518-24. Back to cited text no. 1 |
| 2. | Cosgrove GR, Bertrand G, Fontaine S. Cavernous Angiomas of the Spinal Cord: J Neurosurg 1988;68:31-6. Back to cited text no. 2 |
| 3. | Annand S, Puri V, Sinha S, Malhotra V. Intramedullary cavernous haemangioma. Neurol India 2001;49:401-3. Back to cited text no. 3 |
| 4. | Fortuna L, Palma L, d' Addetta R, Mastronardi L, Acqui M, Foortuna A. Intracranial cavernous angioma. Neurosurg Rev 1992;15:125-33. Back to cited text no. 4 |
| 5. | Moran NF, Fish DR, Kitchen N, Shorvon S, Kendall BE, Stevens JM. Supratentorial cavernous haemangiomas and epilepsy: A review of the literature and case series. J Neurol Neurosurg Psychiatry 1999;66:561-8. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Liscak R, Vladyka V, Simonova G, Vymazal J, Novotny J Jr. Gamma knife radiosurgery of the brainstem cavernomas. Minimally Invasive Neurosurg 2000;43:201-7. Back to cited text no. 6 [PUBMED] |
| 7. | Regis J, Bartolomei F, Kida Y, Kobayashi T, Vladyka V, Liscak R, et al: Radiosurgery for epilepsy associated with cavernous malformation: Retrospective study in 49 patients. Neurosurgery 2000;47:1091-7. Back to cited text no. 7 |
| 8. | Schrottner O, Unger F, Eder HG, Feichtinger M, Pendi G. Gamma-Knife radiosurgery of mesiotemporal tumour epilepsy observations and long-term results. Acta Neurochir Suppl 2002;84:49-55. Back to cited text no. 8 |
| 9. | Hayman LA, Evans RA, Ferrel RE. Familial cavernous angiomas: Natural history and genetic study over a 5-year period. Am J Med Genet 1982;11:147-60. Back to cited text no. 9 |
| 10. | Bicknell JM, Carlow TJ, Kornfeld M. Familial cavernous angiomas. Arch Neurol 1978;35:746-9. Back to cited text no. 10 |
| 11. | Labaque P, Laberge S, Brunereau L, Levy C, Tournier-Lasserve E. Hereditary cerebral cavernous angiomas. Clinical and genetic features in 57 French Families. Societe de Neurochirurgie: Lancet 1998;12:1892-7. Back to cited text no. 11 |
| 12. | Gazzaz M, Sichez J, Capelle L, Fohanno D. Recurrent bleeding of thalamic cavernous angioma under hormonal treatment. Neurochirurgie 1999;45:413-6. Back to cited text no. 12 [PUBMED] [FULLTEXT] |
| 13. | Pozatti E, Acciarri N, Tognetti F, Marliani F, Giangaspero F. Growth, subsequent bleeding, and de novo appearance of cerebral cavernous angiomas. Neurosurgery 1996;38:662-70. Back to cited text no. 13 |
| 14. | Pozatti E, Giangaspero F, Marliani F. Occult cerebrovascular malformations after irradiation. Neurosurgery 1996;39:677-84. Back to cited text no. 14 |
| 15. | Rigamonti D, Spetzler RF, Johnson PC, Dryer BP, Carter LP, Uede T: Cerebral vascular malformation. BNI 1987;3:18-28. Back to cited text no. 15 |
| 16. | Robinson JR, Awald IA. Clinical spectrum and natural course. In Awald IA, Barrow DI, editors. Cavernous malformations. Park Ridge, III: American Association of Neurological Surgeons; 1993;25-36. Back to cited text no. 16 |
| 17. | Brunken M, Sagehorn S, Leppien A, Muller-Jensen A, Halves E. De Novo formation of a cavernoma in association with a performed venous malformation during immunosuppresive treatment. Zentrable Neurochir 1999;60:81-5. Back to cited text no. 17 [PUBMED] |
| 18. | Amirjamshidi A, Abbassioun K. Radiation-induced tumors of the cenral nervous system occuring in childhood and adoloscence. Four unusal lesions in three patients and review of the literature. Childs Nerv Syst 2000;16:390-7. Back to cited text no. 18 [PUBMED] [FULLTEXT] |
| 19. | Curling O Jr, Kelly DL Jr, Elster AD, Craven TE. An analysis of the natural history of cavernous angiomas. J Neurosurg 1991;75:702-8. Back to cited text no. 19 [PUBMED] |
| 20. | Greenberg MS. Handbook of Neurosurgery. Vascular Malformations. New York: Medical Publishers; 2001:804-14. Back to cited text no. 20 |
| 21. | Porter PJ, Willinsky RA, Harper W, Wallace MC. Cerebral cavernous malformations: Natural history and prognosis after clinical deterioration with or without hemorrhage. J Neurosurg 1997;87:190-7. Back to cited text no. 21 [PUBMED] |
| 22. | Giombini S, Morello G. Cavernous angiomas of the brain. Account of fourteen personal cases and review of the literature. Acta Neurochir 1978;40:61-82. Back to cited text no. 22 [PUBMED] |
| 23. | Scott WA, Huy M.Do. Intracranial vascular malformation, and aneurysms. In: Magnetic resonance imaging of the brain and spine. 3rd Ed. Philedelphia: Lippincott Williams & Wilkins; 2002;867-71. Back to cited text no. 23 |
| 24. | Gomori JM, Grossman RI, Goldberg HI. Occult cerebral vascular malformations: Highfield MR imaging. Radiology 1986;158:707-13. Back to cited text no. 24 |
| 25. | Savoiardo M, Strada L, Passerini A. Intracranial cavernous hemangiomas: Neuroradiologic review of 36 operated case. Amer J Neuroradiol 1983;4:945-50. Back to cited text no. 25 |
| 26. | Di Tullio MV Jr, Stern WE. Hemangioma calcificans. Case report of an intraparenchymatous calcified vascular hematoma with epileptogenic potential. J Neurosurg 1979;50:110-4. Back to cited text no. 26 |
| 27. | Ksantikul V, Wirt TC, Allen VA, Netzky MG. Identification of a brain stone as calcified hemangioma: Case report. J Neurosurg 1980;52:862-6. Back to cited text no. 27 |
| 28. | Marra A, Dario A, Scamoni C, Dorizzi A. Intracranial aneurysm associated with cerebral cavernous angioma. Case Report. J Neurosurg Sci 1993;37:25-7. Back to cited text no. 28 |
| 29. | Gastaut JL, Bartolomei F. Partial epilepsy and corpus callosum involvement: Rev Neurol 1993;149:416-8. Back to cited text no. 29 |
| 30. | Hassler W, Zentner J, Peterson D. Cavernous angioma of the optic nerve. Case report. Surg Neurol 1989;31:444-7. Back to cited text no. 30 |
| 31. | Hassler W, Schaller C, Faraghaly F, Rohde V. Transconjuctival approach to a large cavernoma of the orbit: Neurosurgery 1994;34:859-61;discussion 861-2. Back to cited text no. 31 |
| 32. | Musumeci A, Cristofori L, Bricolo A. Persistent hiccup as presenting symptom in medulla oblongata cavernoma. A case report and review of the literature. Clin Neurol Neurosurg 2000;102:13-7. Back to cited text no. 32 |
| 33. | Bristot R, Santoro A, Fantozzi L, Delfini R. Cavernoma of the cavernous sinus: Case report. Surg Neurol 1997;48:160-3. Back to cited text no. 33 |
| 34. | Schmitt JJ, Ebner A. Anatomic substrate of epigastric aura: Case report. Nervenartz 2000;71:485-8. Back to cited text no. 34 |
| 35. | Nieto J, Hinojosa J, Munoz J, Esparza J, Ricoy R. Intraventricular cavernoma in pediatric age. Childs Nerv Syst 2003;19:60-2. Back to cited text no. 35 |
| 36. | Muzumdar DP, Misra BK, Bhaduri AS. Pineal region cavernoma. Case Report: Neurol Med Chair 2000;40:372-9. Back to cited text no. 36 |
| 37. | Muzumdar DP, Bhatjiwale MG, Goel A, Doshi P. Cavernous haemangioma in the interpediuncular cistern: Case report and review of literature. J Postgrad Med 2001;47:191-3. Back to cited text no. 37 |
| 38. | Goel A, Achwai S, Nagpal RD. Dural cavernous haemangioma of posterior cranial fossa. J Postgrad Med 1993;39:222-3. Back to cited text no. 38 |
| 39. | Mottolese C, Hermier M, Stan H, Jouvet A, Saint-Pierre G, Froment JC, et al. Central nervous system cavernomas in the pediatric age group. Neurosurg Rev 2001;24:55-71. Back to cited text no. 39 |
| 40. | Cedzich C, Pechstein U, Zentner J, Van Roost D. Minimally invasive stereotactically-guided extirpation of brain stem cavernoma with the aid of electrophysiological methods. Minimal Invasive Neurosurg 1999;42:41-3. Back to cited text no. 40 |
| 41. | Margolis G, Odom GL, Woodhall B. Further experiences with small vascular malformations as a cause of massive intracerebral bleeding. J Neuropathol Exp Neurol 1961;20:161-7. Back to cited text no. 41 |
| 42. | Hasegawa T, McInery J, Kondziolka D, Lee JYK, Flickenger JC, Lunsford LD. Long-term results after stereotactic radiosurgery for patients with cavernous malformations. Neurosurgery 2002;50:1190-8. Back to cited text no. 42 |
| 43. | Kim DG, Choe WJ, Paek SH, Chung HT, Kim IH, Han DH. Radiosurgery of intracranial cavernous malformations. Acta Neurochir (Wien) 2002;144:869-78. Back to cited text no. 43 |
| 44. | Kondziolka D, Lunsford LD, Flickinger JC, Kestle JR. Reduction of hemorrhage risk after stereotactic radiosurgery for cavernous malformations. J Neurosurg 1995;83:825-31. Back to cited text no. 44 |
| 45. | Pollock BE, Garces YI, Stafford SL, Foote RL, Schomberg PJ, Link MJ. Stereotactic radiosurgery for cavernous malformations. J Neurosurg 2000;93:987-91. Back to cited text no. 45 |
| 46. | Zang N, Pan L, Wang BJ, Wang EM, Dai JZ, Cai PW. Gamma knife radiosurgery for cavernous haemangiomas. J Neurosurg 2000;93:74-7. Back to cited text no. 46 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04150f1.jpg]
[ni04150t2.jpg]
[ni04150t1.jpg]
[ni04150f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}