 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
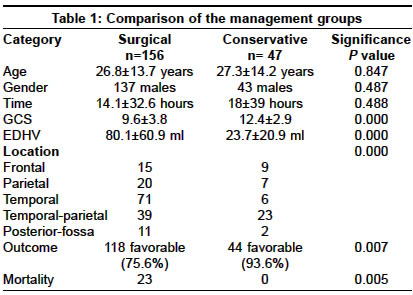
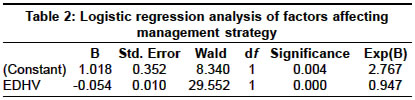
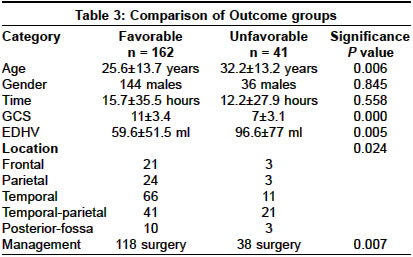
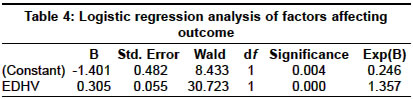
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 443-445 Original Article Does volume of extradural hematoma influence management strategy and outcome? Dubey Arvind, Pillai ShibuV, Kolluri SastryVR Department of Neurosurgery, National Institute of Mental Health and Neurosciences, Bangalore - 560029 Code Number: ni04151 ABSTRACT AIMS: To evaluate the management strategy of extradural hematomas (EDH), particularly with respect to its volume.METHODS AND MATERIALS: Two hundred and three patients with EDH and no other significant intracranial injuries were treated over a period of three years. RESULTS: The factors influencing management strategy and outcome were the Glasgow coma scale (GCS), volume of extradural hematoma (EDHV) and its location. The ultimate clinical outcome was significantly better in patients having EDHV of less than 30 ml. CONCLUSIONS: The key factors influencing the management strategy and clinical outcome are EDHV and GCS at the time of admission. A patient with EDH should not be considered for conservative management if EDHV is more than 30 ml and GCS is 13 or less. Key Words: Extradural hematoma, head injury, Glasgow coma scale INTRODUCTION Several reports have documented the possibility of safely managing patients with extradural hematoma (EDH) without surgery.[1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11] The volume of EDH which has been considered safe for conservative management has ranged from 10 ml to 55 ml in various reports.[5],[6],[8],[10] Both, volume of EDH and the neurological status of the patient have been reported to influence outcome following EDH.[3],[4],[12],[13],[14],[15],[16] Some authors have found that the volume of EDH has no influence on outcome.[17],[2] We aimed to evaluate our current management strategy of dealing with EDH, particularly with respect to its volume. MATERIALS AND METHODS This is a retrospective analysis of 203 patients treated for EDH at our Institute over a period of three years. Patients with significant additional intracranial injuries like contusion, subdural or intracerebral hematoma were excluded from the analysis. Clinical details which were recorded included age of the patient, time from injury to management which was either surgery or start of conservative management (Time), Glasgow coma score (GCS)[18] after resuscitation and the outcome at one to two weeks after injury. Outcome was classified as favorable if the patient was normal or had moderate disability but was independent, and as unfavorable if the patient was not independent. The volume of the EDH (EDHV) was calculated using the Peterson and Espersen equation[19] - a x b x c x 0.5, where a, b, and c represented diameters of the hematoma in the sagittal, axial and coronal planes. The location of the EDH was classified into five groups: frontal, parietal, temporal, temporal-parietal and posterior-fossa depending on the location of the majority of the EDH. The differences between the two management groups (surgery versus conservative) and the two outcome groups (favorable versus unfavorable) were analyzed using the Chi-square test and the Student′s unpaired t-test (two-tailed). RESULTS Two hundred and three consecutive patients with EDH alone were managed over a period of three years. One hundred and fifty-six patients underwent a craniotomy or a craniectomy and evacuation of the hematoma. Forty-seven patients were managed conservatively. The details and comparison of the patients in the two groups are presented in [Table - 1]. The GCS of patients who were managed conservatively was higher and the EDHV lower than those managed surgically. Patients with a temporal or posterior-fossa EDH were more often managed surgically. The two patients with a posterior-fossa EDH who were managed conservatively had EDHV of 8 ml. The stepwise logistic regression analysis reveals that EDHV is the most important factor influencing management [Table - 2]. The details and comparisons of patients in the two outcome groups are presented in [Table - 3]. The most significant factors associated with unfavorable outcome were higher age, lower GCS, and higher EDHV. Posterior-fossa and temporal-parietal hematomas had worse outcome compared to hematomas in other locations. Patients who were managed conservatively had a better outcome than the surgically managed patients. When these factors were entered in a stepwise logistic regression analysis with outcome as the dependent variable, GCS was found to be the most important factor influencing outcome [Table - 4]. The outcome of patients with EDHV above and below 10 ml and every additional 5 ml above that was analyzed and only at and above 30 ml was there a significant difference in outcome [Table - 5], P=0.04). The proportion of unfavorable outcomes was higher in the >30 ml group. DISCUSSION Our analysis has identified GCS, EDHV and location of EDH as the factors that influenced the management strategy. It was observed that the outcome was better in patients with an EDHV of less than 30 ml compared to those with more than 30 ml. This finding corroborates the finding of Bezircioglu et al[5] that patients with an EDHV less than 30 ml could be treated conservatively except when they were temporal in location with a heterogeneous density and the CT was performed less than six hours after trauma. Chen et al[8] reported that supratentorial EDH with volume more than 30 ml, a thickness more than 15 mm and a midline shift more than 5 mm tended to require surgery. Bullock et al[6] managed 12 patients with EDH volume 12-38 ml, conservatively. All the patients were conscious, had no history of deterioration of consciousness, and CT showed the midline shift to be less than 15 mm and basal cisterns were not effaced. Giordano et al[10] reported that patients with a few mild symptoms like headache which was regressing and EDHV less than 55 ml may be managed conservatively. The present analysis has not addressed the issue of posterior-fossa EDH because of inadequate sample size. Wong et al[9] have recommended that posterior-fossa EDH with EDHV less than 10 ml, a thickness less than 15 mm and midline shift less than 5 mm could be managed conservatively. Heinzelmann et al, Mohanty et al, and Kuday et al have reported that lower GCS correlated with a more unfavorable outcome.[12],[15],[13] Rivas et al[3] found that unfavorable outcome was determined by rapid clinical deterioration and EDHV of more than 150 ml. Lobato et al, Lee et al and Servadei et al have reported that outcome was influenced by GCS and EDHV among other factors.[4],[14],[16] In contrast, van den Brink et al[17] found no correlation between EDHV and GCS, and outcome at six months. Paterniti et al[2] reported that when an EDH was operated within six hours then EDHV did not correlate with outcome. We observed that the GCS was the single most important predictor of outcome. Factors like gender, and time from injury to management had no influence on outcome. It appears that the adoption of appropriate criteria to select patients for conservative or surgical management can help avoid unnecessary surgery without affecting the outcome. The main drawback of our study is that only the early outcome was used for analysis because of difficulty or inability to have a longer follow-up on each patient. This probably has resulted in a higher number of patients (n=18) being categorized as severely disabled. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04151t2.jpg] [ni04151t5.jpg] [ni04151t4.jpg] [ni04151t3.jpg] [ni04151t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}