 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
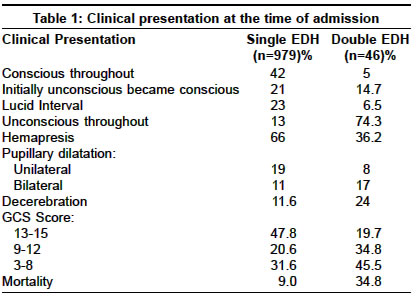
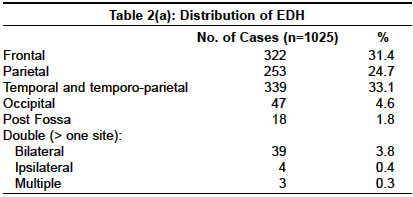
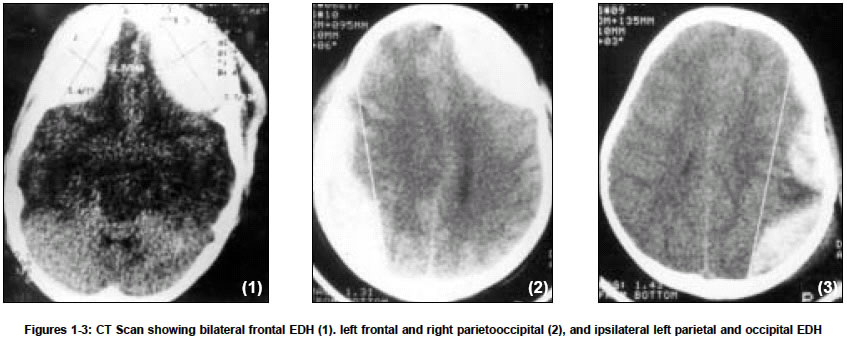
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 450-452 Original Article Double extradural hematoma: An analysis of 46 cases Huda MF, Mohanty S, Sharma V, Tiwari Yogesh, Choudhary A, Singh VP Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221005 Code Number: ni04153 ABSTRACT AIMS: The authors analyze epidemiology, location, clinical profile and outcome of double extradural hematoma (EDH) or EDH at more than one site.DESIGN: A retrospective clinical study. MATERIALS AND METHODS: 46 cases of double EDH were studied. All the cases were evaluated for their mode of injury, clinical presentation, level of sensorium at the time of injury, CT scan finding and outcome after surgery, and were compared with single EDH cases. RESULTS: Out of 1025 cases 46 cases had 'double' EDH. There was bilateral EDH in 39 cases; multiple EDH in 3 cases and ipsilateral double EDH was present in 4 cases. The most common site was frontal (70%). The majority of the patients (80.3%) were in altered sensorium from the time of injury, similar situation was seen in 52.2% of cases with single EDH. The number of patients having a low GCS score was higher when first examined in the double EDH group and the mortality rate was 34.8% as compared to 9% in the single EDH group. CONCLUSION: Majority of the double EDH cases presented with a low GCS and there was a relatively quick neurological deterioration in these cases. Key Words: Double extradural hematoma, head injury, CT scan. INTRODUCTION Double acute extradural hematoma (EDH) was rarely detected before the introduction of computed tomography (CT). Roy (1884) reported the first case of bilateral EDH.[1] Only isolated cases were described prior to 1980 and most of these were diagnosed at autopsy.[2],[3] Double EDH may be unilateral or bilateral. The incidence varies from 2 to 25% of all EDHs in different series and its presence at more than two sites is rare.[4] Incidence of double EDH in children is rarer and our literature search revealed reports of five such cases.[4] We retrospectively analyzed our cases with ′double′ acute EDH. MATERIALS AND METHODS Between 1984 and 2003, 1025 cases with EDH were surgically treated in our neurosurgical department. All the cases were examined clinically and plain computerized tomography scan of the head was performed. RESULTS Double EDH was found in 46 patients (4.48%). These cases were in the age group of 2 to 85 years, mean age being 29 years. Five cases were in the age group of 2-12 years. 72% were males and 28% were females. Vehicular accident was the cause of head injury in 67.4% of cases. In the pediatric age group fall from a height was found in 80% cases. The clinical state at the time of neurological examination is shown in [Table - 1]. The site of hematoma is shown in [Table - 2a, 2b] [Figure - 1], [Figure - 2], [Figure - 3]. The mortality in single EDH patients was 9% while it was 34.8% in patients having double EDH. The mortality was significantly higher in patients who sustained vehicular accident and in those having subdural or intracerebral clots. There was no mortality in patients whose GCS score was between 13-15. In patients with GCS score between 3-8, the mortality was 47.6% in cases with double EDH as compared to 25% in patients with single EDH. Out of 46 patients with double EDH, 39 patients with bilateral EDH underwent surgical evacuation on both sides. Of these, 13 patients died (33%) and the rest clinically improved. Three patients with multiple EDH underwent evacuation of the clot from more than two sites. One of these patients improved and two patients died. Of the four patients operated for ipsilateral double EDH, three patients recovered and one died. DISCUSSION Among the EDH cases the incidence of bilateral EDH has been reported in various studies ranging from 2-25%[5],[6],[7],[8],[9],[10] while its presence at more than two sites is extremely rare. It has been suggested that the force of impact to the head could produce bilateral hematomas, which is more predominant in the anteroposterior direction than from the lateral direction.[11] This is probably the reason for a higher frequency of EDH in the frontal region. In our series 70% patients had frontal EDH and 30% patients had bilateral EDH. Patients with double EDH less frequently have a lucid interval, have a lower GCS, lateralization is frequently absent and deteriorate more often than individuals with unilateral hematomas.[11],[12] Similar features were observed in our series. There were two types of bilateral EDH. In the commoner first type, the bleeding is venous in nature and occurs as a delayed phenomenon, while in the second type the bleeding is arterial in nature.[11],[13],[14],[15] The overall mortality in this series is 34.8% in the double EDH group as compared to 9% in the single EDH group. Gorgulu reported 15.7% mortality in his study of 19 cases of bilateral EDH when the diagnosis was made within 6 hours in 80% of the cases.[16] ACKNOWLEDGEMENT The authors thank Mr. Raghvendra Pandey for assistance in the preparation of the article. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04153t2b.jpg] [ni04153t2a.jpg] [ni04153f1-3.jpg] [ni04153t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}