 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
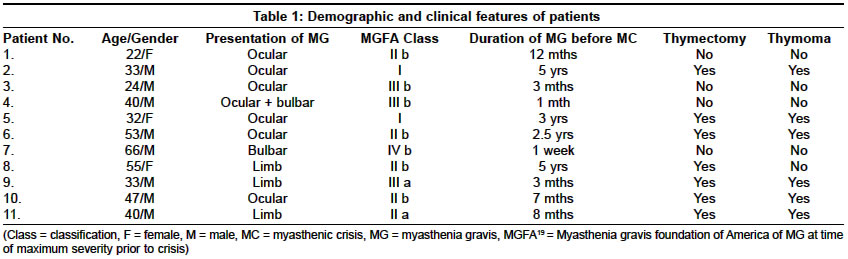
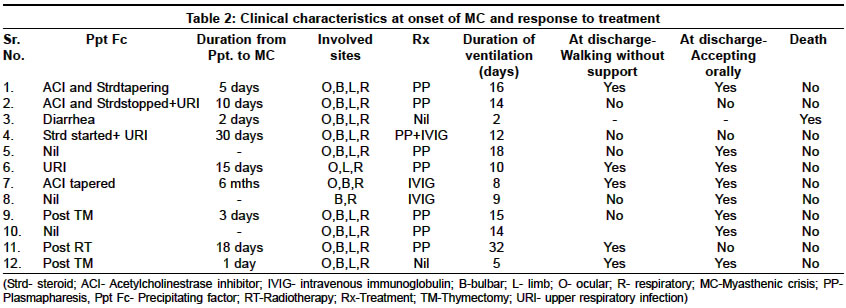
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 453-456 Original Article Myasthenic crisis: A retrospective study Panda S, Goyal Vinay, Behari M, Singh S, Srivastava T Department of Neurology, All India Institute of Medical Sciences, New Delhi Code Number: ni04154 ABSTRACT BACKGROUND AND OBJECTIVE: Myasthenic crisis (MC) is one of the important and common complications in the natural history of myasthenia gravis (MG). MC can be precipitated by multiple factors including deficiency or excess of the acetylcholinesterase inhibitors (AChEI). Any episode of MC is an emergency requiring aggressive therapy. We studied the demographic, clinical and treatment-related characteristics of patients who developed MC.MATERIALS AND METHODS: A retrospective study was conducted in patients with MC admitted during a 31-month period from February 1999 to August 2001, at a tertiary care center in India. RESULTS: Eleven patients (9.69% of the total 114 patients with MG) were admitted with 12 episodes of MC. Mean age at presentation was 39.83 ± 13.18 years with male predominance. Seven patients had undergone thymectomy previously; of which 2 had postoperative MC. Six patients had thymoma. Steroid or cholinesterase inhibitor withdrawal and infections were the commonest precipitating factors for MC. Patients required ventilatory support for median 14 days. They responded to low volume of plasma exchange (PE) (mean 854 ml / day with mean 6.5 cycles per patient). CONCLUSIONS: This report highlights that the subset of Indian patients with MG who are at risk to develop MC belong to the 3rd and 4th decade, have bulbar symptoms at presentation and are associated with thymoma. Patients with MC should have judicious drug adjustments under supervision and should be treated aggressively during impending MC. Key Words: Myasthenia gravis, myasthenic crisis, thymoma. INTRODUCTION Myasthenia gravis (MG), an acquired disorder of neuromuscular transmission, has a prevalence of 0.5-12.5 per 100,000 and an incidence of 0.4 per 100,000 in the general population[1],[2] with a male to female ratio of 2:3.[3] The exact prevalence of MG in India is not known. Myasthenic crisis (MC) is a life-threatening situation, where the weakness arising from MG is severe enough to cause respiratory failure, necessitating intubation with or without mechanical ventilation. It has been reported in 15-25% of patients of MG.[4],[5] With the advances in critical care neurology, the mortality due to MC has significantly reduced from 30-40% in the 1960s and 1970s to 5-10% at present.[5],[6] This has largely been achieved by improved intensive care facilities, early mechanical ventilation, management of precipitating factors, use of acetylcholinestrase inhibitors (AChEI), steroids, antibiotics, plasmapheresis (PP) and intravenous immunoglobulins (IVIG). There have been no systematic epidemiological studies on the prevalence and demographic characteristics of MC in India. However, it may be speculated that with a higher incidence of infections and delayed access to health care in developing countries, more number of patients with MG develop MC which respond well to aggressive respiratory and immunomodulatory care.[7] This retrospective study reviews the demographic profile, clinical features, outcome and mortality in patients of MC admitted at a tertiary care center in India. MATERIALS AND METHODS The case records of patients admitted to the neurology ward and ICU with the diagnosis of MG from February 1999 to August 2001 were screened and cases of MC identified. The diagnosis of MG was based on evidence of muscle weakness, fatigability and diurnal fluctuation of symptoms, and clinical examination, supplemented by positive decrement response on repetitive nerve stimulation test and improvement with edrophonium or neostigmine testing. MC was defined as an episode of severe myasthenia requiring intubation with or without ventilatory support. As a treatment protocol of the department, patients were intubated if clinical assessment suggested compromised respiratory effort documented by decreased patient comfort with either respiratory rate more than 30 per minute, paradoxical diaphragmatic movements, decreased chest expansion, single breath count less than 10 or arterial blood gases showing drop in oxygen saturation.[8] Patients were weaned off the ventilator once the patient′s respiratory effort was sufficient to maintain adequate oxygenation. The decline in vital capacity below 15 ml/kg and above 25 ml/kg has generally been considered as indication for intubation and extubation, respectively.[9] However, the retrospective nature of this study provided limited information. Case records were scrutinized to identify the cause of MC, antecedent events, therapeutic interventions, duration of ventilatory support, hospital stay and any complications during hospital stay. RESULTS Eleven patients with MG (9.64% of the total 114 patients with MG) had 12 episodes of MC. The mean age at presentation was 39.83 ± 13.18 (range, 22-66) years with male predominance (M:F=3:1). The median duration of disease before presentation as MC was 20.02 ± 22.93 months (median of 8 months and ranged from 7 days to 5 years). The demographic and clinical features of the patients are given in [Table - 1]. Seven patients underwent thymectomy prior to the MC. Two patients had MC immediately after thymectomy in the postoperative period. Histologically, six patients had thymoma, and one patient had thymic hyperplasia. At the time of admission, 75% of the patients were on pyridostigmine while 33% were on neostigmine. Sixty per cent of the patients were on steroids and 42% patients were on azathioprine. The factors which could have potentially precipitated MC were cholinesterase inhibitor and steroid withdrawal (3, 25%), respiratory tract infection (3, 25%), thymectomy (2, 16.6%), gastrointestinal tract infection (1, 8.3%), steroid initiation (1, 8.3%) and radiotherapy (1, 8.3%). Among infections, respiratory tract infections predominated. No definite precipitants could be identified in 3 cases. The clinical features during MC, treatment and response to therapy in these cases are detailed in [Table - 2]. Eight (66.66%) episodes of MC were treated with PP and 3 (25%) episodes with IVIG. One case required PP followed by IVIG due to worsening even after PP. Two cases did not receive any therapy (one patient could be weaned off the ventilator by the third post thymectomy day and the other expired on the second day of admission). As a protocol, PP was done on alternate days by small volume PP involving exchange of 10-20 ml/kg of plasma. The average volume of plasma exchange per cycle was 854 ml (range, 600-980 ml) per day and 6.5 cycles (mean) were given per case (range, 5-11 cycles, 11 cycles in one patient). Perceptible improvement (defined as the point of weaning off the ventilator) was observed after an average of 4.2 cycles. The only side-effect observed during PP was hypotension in one patient. IVIG was given in the dose of 0.4 g/kg/day for 5 days in 3 episodes. Drug holiday of AChEI was given throughout the period of ventilation in all the patients. Azathioprine was continued in the same doses as prior to MC while steroids were optimized to 1 mg/kg in 72.72% (8 patients). The duration of ventilatory support varied from 2-32 days (median 14 days) with median stay in intensive care unit of 17 days (range, 2-44). At the time of discharge, AChEI drugs were increased in 9 patients and azathioprine added in 7 patients. At the time of discharge, 40% could walk unsupported and 70% could feed orally. One patient (previously operated for thymoma and with history of MC) died due to septicemia during the second episode of MC. DISCUSSION Early recognition of MC and its precipitating factors with prompt management of MC is life-saving. This study highlights the characteristics of MC and the treatment response in the Indian context. This is a descriptive study of patients with MC encountered in a tertiary care center in north India. The relatively high proportion of patients with MG and MC reported during this short period is a reflection of the referral bias from a large catchment area. The demographic profile reflects that younger patients in the 3rd and 4th decades developed crisis. Though Werneck et al[10] found the mean age at MC to be 24 years, other studies demonstrated bimodal distribution, with preponderance of female patients in the less than 55 years age group and equal gender predominance in patients more than 55 years of age though an overall female predominance was noted.[5],[6],[11] A reversal of male to female ratio seen compared to previous studies, could be due to the small sample size.[6],[10],[11] The median duration of myasthenic symptoms from onset to first crisis was less than in earlier studies (12 months against 21 months to 5-6 years.[5],[12] However, this is comparable to a study on 73 episodes of MC in which the median interval was 8 months.[9] A lesser time to crisis could be the result of more severe myasthenia due to varied reasons. The majority of our patients had thymoma, which is associated with more severe disease. In addition, respiratory infections and different genetic susceptibility for MC in the Indian population may be contributory.[13] Fewer patients of MG developed MC compared to the reported incidence of 15-25% in myasthenic patients.[5],[6] A strong association was found between severe bulbar symptoms and development of MC in the presence of precipitating factors. This was evident from the fact that at the time of presentation with MC, 9 cases (81.81%) had generalized symptoms and all 11 cases had bulbar symptoms. MC occurs more frequently in patients with generalized weakness (75%) compared to oropharyngeal (20%) and respiratory (up to 5%) weakness alone.[14] A higher incidence of bulbar symptoms compared to Berrouschot et al[14] is probably because more patients (6 out of 11 patients) had thymoma. Amongst patients who had undergone thymectomy, 85% had histologically proven thymoma. The natural history of patients of MG with thymoma is a short, stormy course. They develop more frequent episodes of crisis, respond less adequately to immunosuppression, require aggressive therapy with lesser chances of achieving complete remission and have higher mortality. The association between thymoma and poor prognosis of MG has been well documented.[15],[16] In series of patients with MC, thymoma was present in 32% and 20%.[9],[10] The commonest precipitating factor for MC was drug withdrawal and infections, (especially respiratory infections). This observation is similar to prior series which reported infections to be the major precipitant of crisis.[5],[6],[9],[11],[12] Drug withdrawal, however, was frequent in this study. As most of the patients belonged to poor socioeconomic status, drug non-affordability is a common reason for poor drug compliance. All cases of MC received early mechanical ventilation in ICU settings. The exact ventilatory parameters could not be assessed due to the retrospective nature of the study. However, a combination of early, effective mechanical ventilation, adequate antibiotic therapy and aggressive immunotherapy reduced the duration of MC. Aggressive respiratory intervention comprising use of suction, intermittent positive pressure ventilation, bronchodilator treatment and chest physiotherapy helps shorten the course of MC.[8],[17] Despite of lack of Class I evidence in favor of a specific therapy like PP and IVIG, these treatment modalities are the treatment of choice in MC. Most of the cases received PP due to easy accessibility and low cost (being subsidized at our institute) as compared to IVIG. Low volume (854 ml per cycle) PP and less number of cycles (4.2 cycles/ patient) were sufficient for improvement. Despite the small number of cases, this suggests a trend for lower volume PP to be effective in MC. This is further supported by the fact that the median duration of ventilatory support (14 days) and ICU stay (17 days) in the study was similar to the previously reported duration of 13 and 15 days, respectively.[6],[9] The longest duration of crisis reported till date lasted 661 days.[18] These findings contrast with studies recommending higher volume exchange (1.5-2 liters per cycle).[19] The disability at hospital discharge was considerably reduced suggesting effectiveness of treatment during MC. However, similar to other studies[9],[10] no significant difference was observed in the outcome of MC between thymectomized and non-thymectomized patients and between those with and without thymoma. CONCLUSION In the present study relatively young patients with thymoma, generalized myasthenia and oropharyngeal weakness were predisposed to MC. It is prudent to exercise great care while withdrawing cholinesterase inhibitors and steroids. Similar care is also necessary while introducing steroids in patients with MG. Respiratory infection being a common precipitating factor for MC, early institution of antibiotic therapy is recommended in patients with MG. Though the patients showed a trend for a good response to low volume plasma exchanges, we cannot recommend any treatment-oriented decisions due to the small size of this study. Larger systematic studies should be conducted prospectively to answer these questions. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04154t2.jpg] [ni04154t1.jpg] |
| |||||||||

{kind=link}
{kind=link}