 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
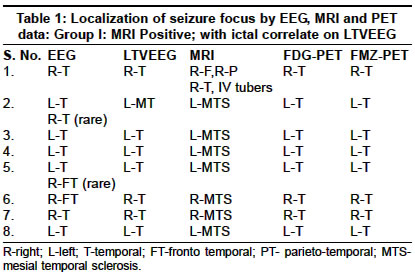
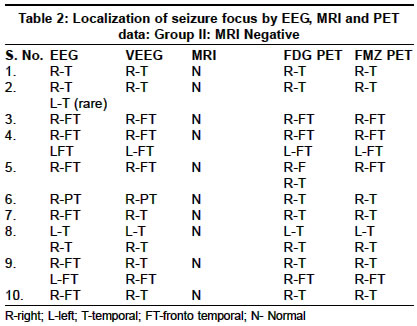
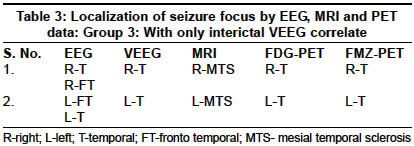
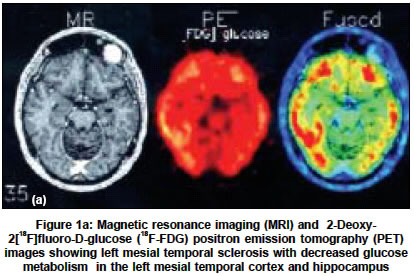
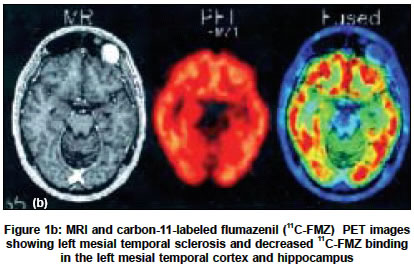
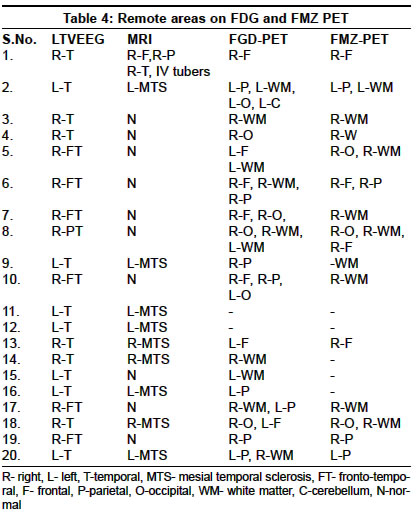
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 457-462 Original Article Clinical utility of 11C-flumazenil positron emission tomography in intractable temporal lobe epilepsy Padma MV, Simkins Robert, White Phillip, Satter Martin, Christian BradT, Dunigan Kelly, Lee Candi, Jacobs M, Mukherjee J, Mantil JosephC Wallace-Kettering Neuroscience Institute, Kettering Medical Center, Wright State University, Kettering, Ohio 45429 Code Number: ni04155 ABSTRACT BACKGROUND: 11C-flumazenil (FMZ) positron emission tomography (PET) is a new entrant into the armamentarium for pre-surgical evaluation of patients with intractable temporal lobe epilepsy (TLE).AIMS: To analyze the clinical utility of FMZ PET to detect lesional and remote cortical areas of abnormal benzodiazepine receptor binding in relation to magnetic resonance imaging (MRI), 2-Deoxy-2 [18F] fluoro-D-glucose, (18F FDG) PET, electrophysiological findings and semiology of epilepsy in patients with intractable TLE. MATERIALS AND METHODS: Patients underwent a high resolution MRI, prolonged Video-EEG monitoring before 18F FDG and 11C FMZ PET studies. Regional cortical FMZ PET abnormalities were defined on co-registered PET images using an objective method based on definition of areas of abnormal asymmetry (asymmetry index {AI}>10%). SETTINGS AND DESIGN: Prospective. STATISTICAL ANALYSIS: Student's "t" test. RESULTS: Twenty patients (Mean age: 35.2 years [20-51]; M:F=12:8) completed the study. Mean age at seizure onset was 10.3 years (birth-38 years); mean duration, 23.9 years (6-50 years). Concordance with the MRI lesion was seen in 10 patients (nine with hippocampal sclerosis and one with tuberous sclerosis). In the other 10, with either normal or ambiguous MRI findings, FMZ and FDG uptake were abnormal in all, concordant with the electrophysiological localization of the epileptic foci. Remote FMZ PET abnormalities (n=18) were associated with early age of seizure onset (P=0.005) and long duration of epilepsy (P=0.01). CONCLUSIONS: FMZ-binding asymmetry is a sensitive method to detect regions of epileptic foci in patients with intractable TLE. Key Words: temporal lobe epilepsy (TLE), intractable TLE, 11C-Flumazenil positron emission tomography (PET), PET, magnetic resonance imaging (MRI). INTRODUCTION Medically intractable epilepsy is frequently associated with structural lesions of the brain, which now can be reliably detected by magnetic resonance imaging (MRI) in an increasing percentage of cases.[1],[2],[3] Although the presence of a lesion predicts better surgical outcome,[4] lesionectomy fails to eliminate seizures in a considerable number of patients.[5],[6] The results are less favorable in extratemporal epilepsies. One of the major reasons for surgical failure is that the epileptic cortex frequently extends beyond the visualized lesion. Remote epileptogenic areas non-contiguous with the lesion may also occur and may be easily missed.[7] 2-Deoxy-2-[18F]fluoro-D-glucose (FDG) positron emission tomography (PET) is a valuable non-invasive method to show focal metabolic abnormalities. The hypometabolic regions are however, commonly larger than the epileptic areas.[8],[9],[10] In in vivo studies of patients with temporal lobe epilepsy (TLE), carbon-11-labeled flumazenil (11C-FMZ) binding has been shown to be reduced in the medial temporal lobe correlating with the epileptogenic area.[11],[12] However, most in vivo 11C-FMZ PET studies have been performed in TLE patients with clear hippocampal atrophy on magnetic resonance imaging (MRI). Whether 11C-FMZ PET can also detect lesions in the medial temporal lobe in patients with normal or mild changes in hippocampal quantitative MRI is uncertain.[13] In vivo data of 11C-FMZ binding abnormalities in epileptic patients with acquired brain lesion are, however, limited and also have rarely addressed the extent of perilesional or remote areas of decreased benzodiazepine receptor function.[14],[15],[16] The present study was undertaken to analyze the clinical utility of 11C-FMZ-PET to detect lesional, and remote cortical areas of abnormal benzodiazepine receptor binding in relation to MRI, 18F-FDG PET, electrophysiological findings and clinical characteristics of epilepsy in patients with intractable TLE. MATERIALS AND METHODS Consecutive adult patients with intractable TLE, under evaluation for possible pre-surgical assessment who gave informed consent were included in the study. The study period was from September 2001 to October 2002. EEG evaluation Nineteen patients underwent prolonged video-EEG recordings and eleven had additional sphenoidal electrode studies. Ictal recordings were obtained in 18 patients. Four patients had depth electrode studies. After MRI, all patients underwent 18F-FDG PET as well as subsequent 11C-FMZ PET examination. The interval between the 18F-FDG and 11C-FMZ PET scans varied from 1 day to 1 month. Epilepsy duration was defined in years as the period between the onset of habitual seizures and the date of the PET examination. A mean yearly seizure frequency before the PET scan was obtained from interviews and medical charts. An estimated lifetime seizure number was then calculated by multiplying the yearly seizure frequency (partial seizures with or without secondary generalization) with the duration of epilepsy. MRI procedure MRI studies were performed on a GE 1.5 T signal 5.6 scanner (GE Medical Systems, Milwaukee, WI). Volumetric imaging was performed utilizing a spoiled gradient echo (SPGR) sequence. The three-dimensional (3D) SPGR sequence generates 124 contiguous 1.5 mm sections of the entire head using a 35/5/1 (repetition time/echo time/ no. of excitations) pulse sequence, flip angle of 35°, matrix size of 256 x 256, and field of view of 240 mm. These images were performed in the coronal plane; the imaging time for this sequence was 9.5 minutes. MRI- based hippocampal and amygdala volumetry was performed by one of the authors in all cases. Axial T2-weighted images were also available in all patients, whereas axial or coronal fluid-attenuated inversion recovery images or both were obtained when the lesion could not be adequately visualized and delineated on the volumetric images. PET Studies The study was ethically cleared by the Institutions′ Research Board (IRB). The PET data was acquired with an EXACT HR± PET scanner (in-plane FWHM=4.6 mm, axial FWHM=3.5 mm, axial FOV=15.52) in 3D mode. For the 11C-FMZ PET study, a 5-minute transmission scan was acquired prior to the administration of the radio-pharmaceutical. Scanning was initiated with a 30-second bolus infusion of 11C-flumazenil (10-20 mCi). The dynamic scanning sequence consisted of 5 frames at 2 minutes and 10 frames at 5 minutes, for a total acquisition time of 60 minutes. The data set was reconstructed using ECAT v7.2 software, using filtered back-projection with a 4 mm Hann filter. The reconstructed data included corrections for attenuation, scatter, normalization and deadtime. Cerebral uptake of intravenously administered 2-Deoxy-2-[18F] fluoro-D-glucose [18F]FDG, 5-10 mCi), prepared according to the method presented by Hamacher et al, occurred while patients lay with eyes open in a dimly lit, quiet room. Emission scanning commenced 40 minutes following the injection of FDG, using a higher resolution Siemens ECAT EXACT HR ± scanner with 3-D mode (CTI PET Systems Inc, Knoxville, Tenn). The patients were placed in the PET camera so as to obtain slices parallel to the cantho-meatal line. Images were reconstructed using a measured attenuation correction and displayed in axial, sagittal and coronal orientations as contiguous planes of brain tissue. All patients had an MRI prior to the PET studies and the PET scans were co-registered with the MRI. Co-registration is currently performed with CRASIS, a fully automated program that we have developed based on mutual information and template-matching. Altogether, 70 to 100 circular regions of interest (ROI) with an average size of 0.5 cm (mediolateral extent) x 2 cm (rostrocaudal extent) were drawn from transaxially cut slices. The brain areas analyzed were the superior, middle and inferior frontal gyrus; the superior, middle and inferior temporal gyrus (referred to as the lateral temporal cortex); the medial temporal lobe (including the hippocampus and amygdala); the parietal and occipital lobes; the white matter and the brainstem. The left/right asymmetry of 11C FMZ binding (asymmetry index = AI%) was calculated for each brain area using the following formula: AI= (L-R)/[L±R]/2). AI greater than 10% was considered significant. The FDG uptake was measured by visual inspection of the PET images and using the metabolic grading: 0= no uptake; 1= uptake less or equal to contra lateral white matter; 2= uptake greater than contra lateral white matter and less than gray matter; 3= equal to or greater than contra lateral gray matter. All the patients with EEG localization to temporal, anterior temporal, and/or mesial temporal were grouped under temporal. Similarly, patients with FDG, FMZ PET localization to mesial temporal, hippocampus, and/or amygdala were grouped under temporal. The investigators of EEG and PET were different. Each of them was blinded to the other′s findings. Analysis of data: The parameters assessed were the concordance (confirming the focus on VEEG, MRI, FDG and FMZ PET studies); visual inspection of areas of abnormal FDG versus FMZ uptake; the presence of remote FMZ and FDG abnormalities and correlation with early age of seizure onset (defined as seizure onset at < 12 years of age) versus late onset (seizure onset at > 12 years of age) and duration of epilepsy (long = > 5 years versus short = < 5 years). The statistical significance of any difference between the two groups in this regard was determined by the student′s "t" test. RESULTS Twenty patients (8 women and 12 men); mean age: 35.2 years; age range: 20 to 51 years) with intractable TLE, who underwent presurgical assessment were evaluated. Anti-epileptic treatment at the time of the PET examinations included mono or polytherapy with phenytoin (n = 8), carbamazepine (n = 10), valproate (n = 5), lamotrigine (n = 7), phenobarbital (n = 1), gabapentin (n = 6), topiramate (n = 4), levetiracetam (n = 5), oxcarbazepine (2), zonisamide (2), felbamate (1). The mean age at seizure onset was 10.3 years (birth to 38 years) and the mean epilepsy duration was 23.9 years. The frequency of seizures varied from once in 4 weeks to several per day. The clinical data and the localization of the seizure focus (i) as shown by the EEG, MRI and the PET data are given in [Table - 1] and [Table - 2]. Electrophysiological correlates of lesional 11C-FMZ PET abnormalities [Table - 3] Nineteen patients had repeated long-term scalp EEG monitoring and long-term video-EEG (LTVEEG) monitoring with scalp, and 11 had additional study with sphenoidal electrodes. Scalp EEGs showed clear, strictly unilateral temporal paroxysmal activity consisting of sharp and slow wave complexes in 13 of the 20 patients and were anteriorly located in 12 patients. Seven patients had bilateral independent, temporal interictal epileptiform activity with a lateralized preponderance. Ictal events with clear, unilateral scalp EEG changes at or before clinical seizure onset, consistent with interictal changes, were observed in 11 patients. Invasive electrophysiological tests were done in four patients. The LTVEEG monitoring studies demonstrated a 100% concordance between the spiking cortex, 18F-FDG PET and the 11C-FMZ PET abnormalities and the mesial temporal sclerosis on the MRI. [Figure - 1a and 1b] show the 18F-FDG and 11C-FMZ PET pictures of a patient with TLE, and left mesial temporal sclerosis on the MRI with glucose hypometabolism and a decreased 11C-FMZ binding in the left mesial temporal cortex and hippocampus. Of the 10 patients with normal MRI, both 11C-FMZ and 18F-FDG PET lateralized and localized the seizure focus concordant with the electrophysiological data. The areas of abnormal 11C-FMZ binding were much more circumscribed as compared to the areas of hypometabolism demonstrated on 18F-FDG PET. A total of 13(65%) and 14(70%) of the 20 patients showed decreased 11C-FMZ binding and decreased glucose metabolism in the ipsilateral thalamus respectively. Occurrence and location of remote PET abnormalities [Table - 4] Remote PET abnormalities were present in 15 patients on 18F-FDG PET and in 18 patients on 11C-FMZ PET. All patients had a long epilepsy duration (85% had seizures for > 10 years; 15% for > 5years and < 10 years). Remote areas of glucose hypometabolism were larger and multilobar in these cases. The remote areas were ipsilateral to the lesion in 10 and contralateral in 5 patients. The remote 11C-FMZ PET abnormalities were smaller than the corresponding remote FDG PET abnormalities and were located in areas having direct corticocortical connections with the primary lesional area and were always ipsilateral. A corresponding area of glucose hypometabolism was seen in the contralateral temporal cortex in 2 patients. A decreased 11C-FMZ binding seen in 5 patients, of these, 3 patients had bitemporal spikes on EEG. Interestingly, (75%) of the patients demonstrated decreased 11C-FMZ binding in the ipsilateral white matter. Also, 4 (20%) patients showed decreased 11C-FMZ binding in the ipsilateral cerebellum. Though not statistically significant, differences were found according to the presence (n = 15; mean age at seizure onset: 6.7±9.7 years; mean epilepsy duration: 13.2±11 years) or absence (n = 5; mean age at seizure onset: 15.7±11.4 years; mean epilepsy duration: 8.6±7.6 years; P=0.512) of remote 18F-FDG PET findings. The mean age at seizure onset was 29 years lower in patients with remote FMZ PET abnormality (7.4±2.1 years) than in those without it (36±1.5 years; P=0.005). There was also a 16 year-difference in the mean duration of epilepsy between these two groups (25 years for patients with and 9 years for patients without FMZ PET abnormality; P=0.01). DISCUSSION Koepp et al, demonstrated significant changes of hippocampal FMZ-Vd (flumazenil volume distribution) in six of eight patients with TLE and normal quantitative MRI.[17],[18],[19] It was also possible to detect areas of abnormal cortical FMZ biding, both decreases and increases, in 12 of 17 patients with extratemporal lobe epilepsy and normal high-quality MRI. Greater reductions of 11C-FMZ binding have been reported in patients with frequent seizures, in comparison with those with less frequent seizures.[7] They had concluded that 11C-FMZ-PET, corrected for partial-volume effect,[20] may be clinically useful in preoperative epilepsy evaluation when quantitative MRI does not reveal a single abnormality that is concordant with other data. Lamusuo et al,[21] demonstrated the mean 11C-FMZ binding in the ipsilateral and also in contralateral medial temporal lobe to be reduced in patients with TLE compared to controls. 11C-FMZ binding in the medial temporal lobe also correlated with the severity of reduced hippocampal volume, T2 prolongation, histopathologically assessed neuronal loss, and astrogliosis. In addition, it was abnormal even in patients with normal or mildly damaged hippocampus on quantitative MRI. They proposed that the loss of granule cells in the dentate gyrus and pyramidal cells in the hippocampus proper mostly contribute to the reduced 11C-FMZ binding. We did not correct our data for partial volume effect, which has been emphasized when quantifying BZ binding obtained with PET in small structures such as the hippocampus.[20] However, to use partial volume correction would be laborious and complicated, and moreover, its clinical utility has not been determined. If we had taken into account the partial volume correction, we would probably have obtained an even more pronounced decrease in 11C-FMZ binding in the ipsilateral medial temporal lobe, but would have obtained increased values of 11C-FMZ binding on the contralateral side. This would have led to a greater asymmetry between the ipsilateral and contralateral side, and thus, some patients with no significant asymmetry in uncorrected 11C-FMZ binding might have had a significant asymmetry in partial volume corrected flumazenil data. Indeed, in a study comparing partial volume corrected and uncorrected flumazenil distribution volumes, more patients were found showing significant asymmetry after using partial volume correction. Thus, 11C-FMZ PET without correcting the partial volume effect may have underestimated rather than overestimated its ability to localize the epileptogenic area. The areas of decreased FMZ binding are in general smaller than the corresponding regions of glucose hypometabolism and might be more specific for the electrophysiologically abnormal cortex in such patients. FMZ PET may assist in surgical planning and may also further localize potentially epileptogenic regions in patients with extensive FDG PET abnormalities. Remote FMZ PET abnormalities The current study demonstrated the occurrence of FMZ PET abnormalities remote from the lesion and the primary epileptic focus in epileptic patients with early onset of seizures as well as relatively long duration of epilepsy. The results of the present study confirm the earlier study by Juhaz et al[22] Ipsilateral remote FMZ PET abnormalities occur especially in patients with seizure onset at an early age. These remote abnormalities potentially represent areas of secondary epileptogenesis as described by Morrell,[23] who also suggested that their removal may not be required to alleviate seizures if they are "dependent" (as compared with "independent" secondary foci, which need to be removed). Remote abnormalities of glucose metabolism are common in partial epilepsies and indicate functional abnormalities that may be reversible. Widespread FMZ PET abnormalities were also previously reported in patients with pure hippocampal sclerosis, with dual pathology as well as with cortical dysgenesis.[24] It was shown in chronic animal models of focal epilepsy that remote spread of electrical and metabolic alterations is not random but depends on the connectivity of the affected epileptogenic area. Consistent with this, a series of patients with temporal lobe epilepsy was recently reported who showed reduced BDZ-R density not only in the epileptogenic temporal regions but also in some of their primary projection areas.[25] Based on electrophysiological data, it was also demonstrated that those patients with brain lesion, who had a remote epileptic focus, had significantly longer duration of seizures than others whose foci were confined to the lesion or to the perilesional cortex. This is consistent with our findings and we suggest that remote areas of decreased BDZ-R binding are secondary to an early-onset long-lasting lesional epilepsy and potentially represent areas of secondary epileptogenesis. In addition, it has already been shown that poor surgical outcome is associated with long duration of epilepsy as well as presence of generalized seizures. Unresected remote epileptogenic areas may be a possible explanation of poor surgical outcome in such cases. It was not possible to address remote 11C-FMZ PET abnormalities by EcoG in our series. Decreased fluamzenil binding and glucose metabolism of the dorsomedial nucleus of the thalamus are common and have strong lateralization value for the seizure focus in human TLE.[11] The current study identified decreased 11C-FMZ binding in the ipsilateral thalamus in 65% of the patients. Decreased 11C-FMZ binding could be due to neuronal loss, as suggested by volume loss, or could also indicate impaired gamma-aminobutyric acid (GABA (ergic) transmission in the dorsomedial nucleus, which has strong reciprocal connections with other parts of the limbic system. Increased glucose metabolism and flumazenil binding in the lateral thalamus representing an upregulation of GABA-mediated inhibitory circuits has been reported in earlier studies.[10] Anti-epileptic medication may have affected 11C-FMZ binding in the current study. A decrease in 11C-FMZ binding in cortical areas that did not contribute to seizure initiation may be due to this phenomenon. However, the effect of the particular drug on 11C-FMZ binding was difficult to study because of the various combinations of drugs and the heterogeneity of patients. The association of reduced 11C-FMZ binding with reduced blood flow due to medication or seizures also seems unlikely as 11C-FMZ binding has been shown not to be affected by blood flow. It has been suggested that seizures affect 11C-FMZ binding. In the current study, the interval between the last seizure and 11C-FMZ PET imaging was at least 24 hours. Localizing the epileptogenic area in patients with unilateral hippocampal damage on quantitative MRI is usually less complicated than in patients with a normal quantitative MRI, who might still benefit from the surgery. One of the most important clinical functions of the pre-surgical procedure is to localize the epileptogenic area accurately enough so that invasive subdural EEG can be eliminated. The results of 11C-FMZ PET may help in the design of subdural EEG recording. In the current study, 11C-FMZ PET helped in investigating the hippocampal damage even in patients with no remarkable hippocampal abnormalities on quantitative MRI. It is known from previous studies that decreased FMZ binding may occur in normal-appearing MRI. These cortical regions may represent regions with abnormal histology and cell loss. In the present study, 11C-FMZ-PET detected functional abnormalities over and above the structural abnormalities revealed by optimal MRI. Ten patients with a normal MRI had a significant unilateral decrease of glucose metabolism and decreased 11C-FMZ binding at the site of the EEG focus. Eight of these had a surgically relevant abnormal FMZ-AI and these were concordant with the presumed epileptic focus on EEG. Different investigators have found a varying yield of surgically relevant unilateral decreases of 11C-FMZ binding in patients with refractory TLE of mixed origin in their comparisons of PET and MRI. Studies comparing different imaging modalities, such as MRI and PET, are subject to bias, because the methodologies and equipment are often not developed to the same degree in any one center. Patients who were previously regarded as being "MRI negative" by one center may have relevant abnormalities identified with contemporary optimal MRI by another center. A difficulty of studying patients with normal MRI is the lack of a gold standard, such as histological verification of hippocampal sclerosis or postoperative seizure control. Ten out of 20 consecutively studied patients with intractable TLE, in the present study had normal qualitative and volumetric MRI. 11C-FMZ-PET and 18F-FDG -PET was abnormal in all 10 of these patients and provided clinically useful, EEG-concordant data. 11C-FMZ-PET and 18-F-FDG - PET therefore detected functional abnormalities over and above the structural abnormalities revealed by optimal MRI. The major limitation in the present study is the lack of surgical correlation. We could not substantiate the localizing value of FDG and FMZ PET in patients with non-localizing MRI nor could we further clarify the clinical importance of distant regions with glucose hypometabolism and abnormal FMZ binding. The surgical outcome of a larger series of patients undergoing cortical resection should be analyzed in future studies. Nevertheless, our results suggest that 11C-FMZ PET and 18F-FDG-PET can provide valuable additional information beyond MRI. We conclude from the current study that both 18F-FDG-PET and 11C-FMZ-PET are useful in localizing the epileptic focus in patients with intractable TLE, including those with a non-localizing high-quality MRI. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04155f1b.jpg] [ni04155t3.jpg] [ni04155t1.jpg] [ni04155f1a.jpg] [ni04155t4.jpg] [ni04155t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}