 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
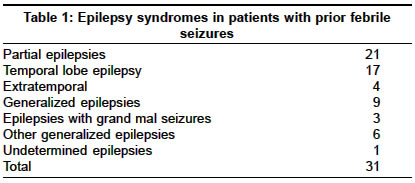
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 463-465 Original Article Adult-onset epilepsy and history of childhood febrile seizures: A retrospective study Mohebbi MohammadR, Navipour Reza, SeyedKazemi Mojdeh, Zamanian Hadi, Khamseh Fatemeh Department of Medical Genetics, Tehran University of Medical Sciences, Tehran Code Number: ni04156 ABSTRACT BACKGROUND: Children with febrile seizures (FS) are at higher risk of developing epilepsy. There is robust literature on epilepsy with onset in childhood following FS but very little on the same issue in adults. Key Words: Partial epilepsy, seizure, febrile seizure, convulsion, unprovoked, genetic. INTRODUCTION Febrile seizures (FS) occur in 2-5% of children.[1],[2] There are hardly any epidemiological studies of febrile seizures in the Iranian population. The study from India by Bharucha et al[3] in the Parsi community (those of Iranian descent) reported a frequency of 1.77%. The reported proportion of children with FS who later developed epilepsy was between 2% and 7%.[4] A considerable number of patients may develop epilepsy after 16 years of age.[5] Certain features of FS may be predictive of a particular type of later epilepsy.[5],[6] Molecular genetic studies to date have found several loci for FS on autosomal chromosomes. Partial seizures have also been linked to regions of autosomal chromosomes.[7],[8] There is robust literature on epilepsy with onset in childhood following FS, but very little on the same issue in adults. In the present study, we evaluated the association between history of childhood FS and adult-onset epilepsy, and also a possible association between history of childhood FS and any specific type of epilepsy and epilepsy syndrome. MATERIALS AND METHODS This was an observational study with no therapeutic interventions or management. The research committee of the faculty of medicine had approved the study. Written informed consent was obtained from all patients aged 18 years and above and in case of patients aged less than 18 years, informed consent was obtained from the parents. The study material included 101 consecutive patients with adult-onset (> 14 years old) unprovoked seizures. Patients were recruited from a referral hospital located downtown in Tehran city, from June 2002 to December 2002. All patients were admitted to the hospital. Detailed history and neurological examination was done in all the patients. The medical records, electroencephalograms, and the neuroimaging data of the patients, available from the medical records department of the hospital, were reviewed and the details of their past and present illness were collected. The authors confirmed data regarding the childhood FS event by interviewing personally (no telephonic interview) the patients′ mothers or sibs. We made every effort to distinguish between ′FS′ and ′seizures with fever′. Seizure with fever was defined as any convulsion in a child of any age with fever of any cause.[9] A single seizure with no focal features and lasting less than 15 minutes in an infant with fever was defined as a simple febrile seizure. Febrile seizure was defined as complex if the above criteria were not fulfilled.[10] The criteria proposed by the International Classification of Seizures[11] and International Epilepsy and Epilepsy Syndromes[12] were considered while classifying the seizure type and epilepsy and epilepsy syndrome. Because of the small number of patients with different epilepsy syndromes, we grouped patients as localization-related, generalized and undetermined epilepsy [Table - 1]. The data were evaluated by Chi-square test and the Mantel-Haenszel method was used to obtain the odds ratios using Statistical Package for the Social Sciences (SPSS Inc. Chicago, Illinois) for Windows version 11.0. A P-value of <0.05 was considered statistically significant. RESULTS Of the 101 patients with adult-onset epilepsy with history of childhood FS, 9 patients were excluded for further analysis for the following reasons: bacterial meningitis (2), recent head trauma (1), brain tumor (2), tricyclic antidepressant overdose (2) and lack of reliable data regarding the childhood FS event (2). The epilepsy categories in the remaining 92 patients [median age: 18 years, range: 14-43] were: localization-related epilepsies in 45 (48.9%), generalized epilepsies in 37 (40.2%), and undetermined epilepsies in 10 (10.9%). Thirty-one patients [22 (71%) men and 9 (29%) women; median age: 24 years, range: 15-43] had history of FS in the childhood. Localization-related epilepsies (n=21) outnumbered generalized epilepsies (n=9) in patients with history of childhood FS, 27 patients had simple FS and 4 had complex FS. Positive history of FS was seen significantly more in men than women [Odds ratio: 2.70; (95% CI, 1.07-6.80)] ( c2= 3.63, df = 1,P=0.035). Comparison between different groups of epilepsy syndromes showed a significant association between localization-related epilepsies and a history of childhood FS [Odds ratio: 3.24; (95% CI, 1.30-8.06)] ( c2= 5.49, df = 1, P=0.012). Similar association was also found between localization-related and generalized epilepsies after we excluded epilepsies in the undetermined categories. [Odds ratio: 0.37; (95% CI, 0.14-0.95)] ( c2= 4.40, df = 1, P=0.039). Age of onset of epilepsy did not differ significantly between the generalized and localization-related epilepsies. Of the 21 patients with localization-related epilepsies, 17 had a simple partial unprovoked seizure as the initial seizure type. Comparing different groups of epileptic seizures (simple partial, complex partial, and generalized), a significant association was found between an initial simple partial unprovoked seizure and a positive history of FS [Odds ratio: 8.05; (95% CI, 2.88-22.45)] ( c2= 15.86, df = 1, P<0.001). No significant association was found between type of the FS and characteristics of the adulthood seizure event, possibly due to the small number of the patients in each group. The age of onset of epilepsy and family history of seizures were not found to be significantly associated with a history of FS. DISCUSSION Children with FS have a genetic predisposition to convulsions in association with fever due to inheritance of a low seizure threshold.[13] Localization-related epilepsies were significantly associated with a history of childhood FS in our study. Perhaps, those genetically susceptible to FS in childhood are more prone to develop localization-related epilepsies in adulthood, or fever may act as a trigger that unmasks a preexisting tendency to epilepsy, which may later manifest itself with febrile seizures. We also found a significant association between a positive history of FS and an initial simple partial unprovoked seizure (with no impairment of consciousness) in adulthood. Associations between complex FS and partial onset unprovoked seizures have been reported in the literature suggesting an underlying brain pathology common to both.[14] Consistent risk factors for the development of unprovoked seizures following a first FS include a family history of epilepsy, complex features of FS, and presence of neurodevelopmental abnormalities present from birth.[15] Children with complex FS have reportedly a higher risk of unprovoked seizures than children with "simple" FS.[15] The majority (87%) of the FS in the present study were of simple type. In a recent study on FS in Tehran,[16] 72% of the 238 consecutive children of 3 months to 5 years old with FS who entered the study in three consecutive years (as a sample of Tehran FS population) were of simple type. Although the frequency of those with a history of simple FS is more in the present study, we found no significant association between the type of the adult-onset epilepsy and the simple or complex features of the childhood FS. Using the Rochester epidemiological project records-linkage system, Annegers et al[15] found that 32 of the 687 children with a first FS developed subsequent unprovoked seizures. Sixteen were partial and 16 were generalized-onset seizures. The incidence of both types of seizures was significantly higher than expected in the Rochester population, but the morbidity ratio for partial epilepsies was greater than that of the generalized-onset seizures.[15] By 10 years of age, there were fivefold more children with unprovoked seizures than expected in the Rochester population. In the follow-up of their patients, the incidence of unprovoked seizures was still five times the general population at the age of 20 years or older.[15] In the study by Trinka et al on 113 adult patients with epilepsy, the majority of them developed epilepsy after age sixteen.[5] The relatively high rate of prior FS in our study is not in agreement with the literature.[4],[15] This can be because of a selection bias in a hospital-based study. This is the inherent weakness of such studies. In a recent retrospective study on 109 epileptic patients with prior FS, Saltik et al suggested that some characteristics of the FS may reflect the type of epilepsy that subsequently develops.[6] The results of the study by Trinka et al support the view that prolonged and lateralized FS are associated with temporal lobe epilepsy, whereas brief and generalized FS are probably an age-dependent expression of seizure susceptibility.[5] Both FSs and epilepsies are regarded as genetic in origin.[7],[8] Generalized epilepsy with FS plus (GEFS±) is also a genetic syndrome characterized by heterogeneous epilepsy phenotypes including FS and mild to severe generalized epilepsies.[17] However, partial epilepsies occur rarely in this setting.[18] According to the Western literature,[8] partial seizures are the most common seizure disorder in adults; in India, however, generalized seizures outnumber other types of seizure.[19] We know much less about the mechanisms underlying partial-seizure disorders than we do about generalized epileptogenesis.[8] By all indications from our study, the significant association between history of FS and occurrence of partial epilepsies warrants more investigation to better understand the mechanism and underlying causes of unprovoked partial epilepsies as well as the possible underlying genetic factors common in both FS and partial epilepsies in the affected probands. ACKNOWLEDGEMENTS We wish to thank Dr. Elham Hatef, M.D., for her kind help with the statistical analysis. We also thank Dr. Bijan Sadri, M.D., for providing the references. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04156t1.jpg] |
| |||||||||

{kind=link}