 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
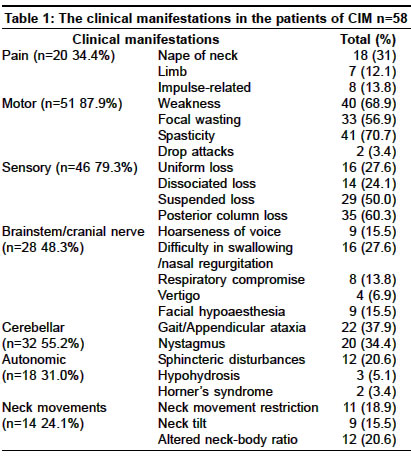
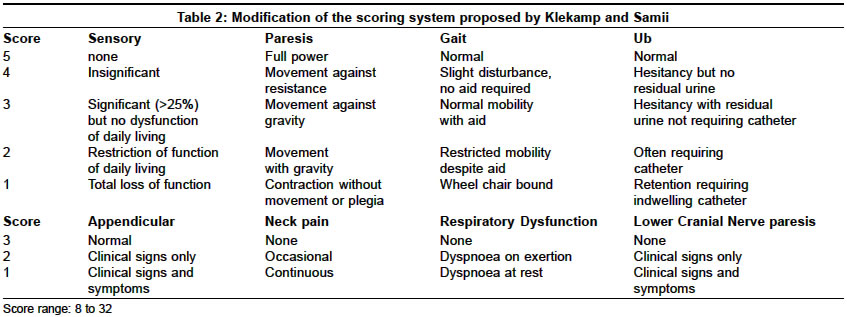
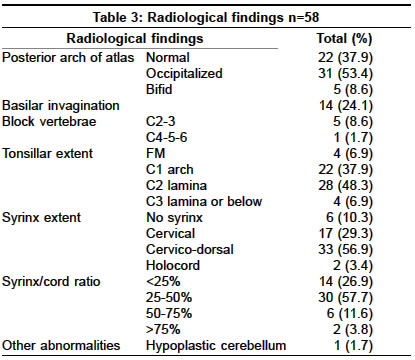
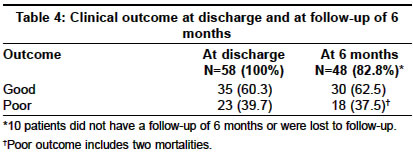
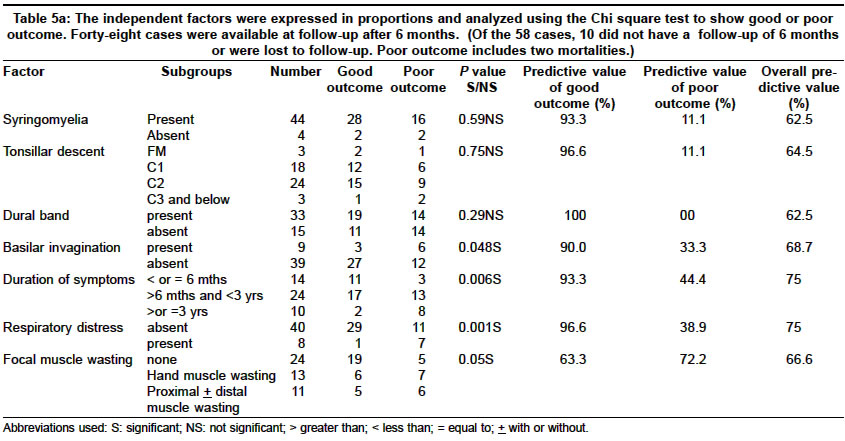
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 470-474 Original Article Factors influencing the outcome in symptomatic Chiari I malformation Arora Pankaj, Behari Sanjay, Banerji Deepu, Chhabra DevendraK, Jain VijendraK Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Rae Bareli Road, Lucknow - 226014 Code Number: ni04158 ABSTRACT BACKGROUND: To study the clinico-radiological determinants of outcome in patients with Chiari I malformation (CIM).MATERIALS AND METHODS: The disability assessment of 48 patients with C I M who underwent posterior decompression was done by modified Klekamp and Samii scoring system. The outcome was regarded as good when the patient was ambulant without any aid with an improvement in the disability score; and, poor when (a) there was postoperative deterioration or lack of improvement; (b) the patient was non-ambulant without aid, irrespective of the improvement in the clinical score; or, (c) there was a perioperative mortality. Patients with hydrocephalus; those who underwent syringo-subarachnoid or syringo-peritoneal shunt as the primary procedure; and, patients with atlanto-axial dislocation were excluded from the study. STATISTICAL METHODS USED: Categorical data were expressed in proportions and analyzed with Chi square test. Analysis of factors predicting clinical outcome at 6 months was done utilizing logistic regression analysis. RESULTS: The outcome assessed at six months showed that 30 patients (62.5%) had good outcome while 18 patients (37.5%; including two perioperative mortalities) had a poor outcome. CONCLUSIONS: Significant predictors of outcome in patients with CIM include the duration of symptoms (P value=0.006), respiratory distress (P value=0.001), and basilar invagination (P value=0.048). The effect of syringomyelia in predicting the clinical outcome could not be determined due to the differences in the number of patients in the groups with or without syringomyelia. Key Words: Chiari I malformation, craniovertebral junction, posterior decompression. INTRODUCTION Chiari I malformation (CIM) refers to the downward herniation of cerebellar tonsils through the foramen magnum (FM).[1],[2],[3] The anomaly is a leading cause of hydrosyringomyelia. Surgery aims at relieving the compression at the cervicomedullary junction, at restoration of the normal cerebrospinal (CSF) flow dynamics across the FM, and in facilitating the resolution of syringomyelia.[2],[3],[4],[5] In this retrospective study, in patients with CIM, with or without syringomyelia, the factors influencing outcome were determined utilizing logistic regression analysis. MATERIAL AND METHODS Fifty-eight consecutive patients (mean age 26.92 years; range 11-64 years; 47 males and 11 females) of CIM underwent posterior decompression between 1991-2001. In 48 patients with CIM (including two perioperative mortalities, 10 patients did not have a 6-month follow-up or were lost to follow-up), a statistical analysis utilizing the clinical status at 6 months was performed. Patients with associated hydrocephalus, those who underwent syringo-subarachnoid or syringo-peritoneal shunt rather than posterior decompression as the primary procedure; and, patients with atlanto-axial dislocation (AAD) were excluded from the study. Spasticity and motor weakness, focal muscle wasting, loss of posterior column sensations, appendicular or gait ataxia, and nystagmus formed the predominant clinical manifestations [Table - 1]. Eight patients also had dyspnoea at rest. A quantitative assessment of the disability of these patients was performed utilizing a modified version of the Klekamp and Samii scoring system.[6],[7] This clinical score ranged from a minimum of 8 to a maximum of 32 [Table - 2]. The original scoring system proposed for syringomyelia[6] was modified to take into account the manifestations of CIM including cerebellar signs, neck pain, respiratory dysfunction and lower cranial nerve paresis.[7] The radiological investigations included plain dynamic radiographs of the cranio-vertebral junction (in flexion and extension) to assess for AAD, basilar invagination (BI), the status of atlas (occipitalized or normal) and Klippel Feil anomaly. A T1- and T2- weighted cranio-spinal magnetic resonance imaging (MRI) was performed to assess the extent of cervicomedullary compression, tonsillar herniation and syringomyelia. Based on MRI, the tonsillar descent was categorized as reaching till a) FM; b) posterior arch of C1; c) lamina of C2; and, d) at or below the lamina of C3. The vertical extent of syrinx, as well the syrinx / cord diameter ratio [using Vaquero′s index[8],[9] were also noted [Table - 3]. The patients underwent posterior decompression in a standard prone position. The surgical treatment included a sub-occipital craniectomy of size 2.5 cm x 2.5 cm that always included the posterior rim of FM. Depending upon the extent of tonsillar descent, a C1, C1-2, or C1-3 laminectomy was performed in 27, 22 and 5 cases, respectively. An autologous fascia lata or cervical fascia was used for duraplasty in 32(55%) and 24(41.4%) patients, respectively; in 2 patients no graft was used. A thickened band-like tissue at the cervico-medullary junction as described by Williams[4],[5] was found in 41 (70.7%) patients. The tonsil was found to be asymmetrical in 7(11%) cases. In addition to the posterior decompression, obex plugging in 4 patients, and syringo-subarachnoid shunt in 1 patient, were performed. The following complications occurred following posterior decompression and duraplasty. Respiratory distress increased in 4 patients with a poor preoperative respiratory reserve, and required tracheostomy and prolonged ventilatory support. Two of these patients subsequently showed improvement. However, one patient with a poor respiratory reserve and lower cranial nerve paresis succumbed to aspiration pneumonitis, while the other patient developed sudden respiratory arrest after discharge from the hospital. Six (10.3%) patients developed CSF leak from the operative wound site of which 2 patients developed meningitis. These patients responded to conservative management and one patient required re-exploration and repair of the defect. In 4 out of the 6 patients, the cervical fascia had been used for duraplasty. Wound infection occurred in 5 patients, and air embolism was seen in 1 patient. The follow-up clinical status after 6 months of surgery was available in 48 patients (10 patients did not have a 6 month follow-up or were lost to follow-up). Categorical data of the seven independent factors were expressed in proportions and analyzed with Chi square test. The analysis of the factors predicting the clinical outcome at 6 months was done utilizing logistic regression analysis. The statistical analyses were performed using the SPSS for Windows software (version 9.0; SPSS, Inc., Chicago, IL). The outcome was regarded as good when the patient was ambulant without any aid and had an improvement in the clinical score; and, poor when a) there was postoperative deterioration or lack of improvement; b) the patient was non-ambulant without aid, irrespective of the improvement in the clinical score; or, c) there was a perioperative mortality [Table - 4]. A univariate analysis was performed taking seven independent factors, namely the duration of symptoms; respiratory distress; focal muscle wasting; the presence of syrinx; dural band; BI; and, the extent of the tonsillar descent [Table - 5a]. Subsequently, a multivariate analysis, using the factors that were found to be significant on univariate analysis, was done [Table - 5b]. A p value of less than 0.05 was considered significant. RESULTS The duration of symptoms in the series varied from 2 months to 15 years with a mean of 2.6 ± 2.3 years and median of 2 years [Table - 1]. The mean modified Klekamp and Samii score for patients of CIM with syringomyelia (Group A; n=52) was 24.2 ± 2.9, and for those without syringomyelia (Group B; n=6), 21 ± 1.3. The incidence of long tract and brainstem signs was high in both the groups. Group A patients had additional features of intramedullary pathology of dissociated or suspended sensory loss and Horner′s syndrome; and, Group B patients presented more often with pain in the nape of the neck, posterior column deficits and cerebellar signs. At follow-up, the mean clinical score of the patients improved from 23.82 ± 2.96 to 25.96 ± 2.1. In Group A, the scores changed from 24.2 ± 2.9 to 26.1 ± 2.1; and in Group B, from 21 ± 1.3 to 24.7 ± 0.8. The major improvements occurred in spasticity (in 34 of the 41 patients, 82.9%); pain in the nape of the neck (in 13 of the 18 patients, 72.2%); and cerebellar signs (in 20 of the 32 patients, 62.5%). The outcome assessed at 6 months in 48 patients showed that 30 (62.5%) had good outcome while 18 (37.5%; including two perioperative mortalities) had a poor outcome [Table - 4]. At a follow-up of 6 months, the factors, duration of symptoms (P value=0.006), respiratory distress (P value=0.001), focal muscle wasting (P value=0.053) and BI (P value=0.048) were found to be predictors of outcome on univariate analysis. On multivariate analysis using these 4 factors, the significant factors predicting clinical outcome were BI, duration of symptoms and respiratory distress while focal muscle wasting was not found to be a significant predictor of the clinical outcome. This model correctly predicts a good outcome in 90.0% of the cases and a poor outcome in 72.2% patients. The overall predictive value with all the four factors was 83.3% (P value=0.004); the predictive value taking the three factors, namely basilar invagination, duration of symptoms and respiratory distress was again 83.3% (P value 0.002). Thus, focal muscle wasting was not found to be a significant predictor of outcome [Table - 5a and 5b] . DISCUSSION In the present series, the patients with CIM without syringomyelia had FM compressive symptoms and signs rather than the central cord symptomatology seen in patients with syringomyelia, as also noted by Pillay et al.[10] Following posterior decompression and duraplasty, the improvement in the long tract signs was less marked in patients with syringomyelia due to the persistence of syringomyelia that takes a long time to recover.[11] According to Pillay et al, the presence or absence of syringomyelia seemed to be the main determinant influencing the surgical outcome.[10] Levy et al[12] and Saez et al[13] have reported poor results in patients with a central cord syndrome as opposed to patients with a cerebellar syndrome. In our statistical analysis, due to the differences in the number of patients in the two groups (44 versus 4 patients), the effect of syringomyelia in determining outcome could not be ascertained. The authors relied mainly on posterior decompression and duraplasty as the procedure for relieving both the clinical manifestations of CIM and syringomyelia. The craniocervical posterior decompression and duraplasty removed the block at FM and re-established the normal communication between the cranial and spinal subarachnoid spaces. This led to a simultaneous relief of pressure of the tonsils on the cervicomedullary junction as well as to the amelioration of the factors responsible for the development of syringomyelia.[2],[3],[6],[14],[16],[17],[18] In this retrospective study, the patients with CIM with associated BI also underwent only posterior decompression; and, some patients with CIM and syringomyelia underwent an additional obex plugging or syringoperitoneal shunt after posterior decompression. Both these categories of patients were included in the study since they all underwent posterior decompression as the primary procedure for CIM. Many authors have recognized the prognostic value of certain clinical variables in CIM. Poor outcome is frequently observed in patients with signs or symptoms suggestive of syringohydromyelia,[2],[10],[12],[19] atrophy, ataxia and nystagmus.[2] Some authors have associated patients having prolonged symptoms with poor outcomes[10],[19] but others have not.[20] Dyste et al have proposed a less favorable outcome in patients with muscle atrophy, symptoms longer than 24 months, ataxia, nystagmus, trigeminal hypoaesthesia and dorsal column dysfunction and have proposed a statistical model based on atrophy, ataxia, and scoliosis that allows prediction of the long-term outcome at 95% confidence level.[2] In the present series, a few new independent factors like respiratory dysfunction, basilar invagination, extent of tonsillar descent and the dural band were assessed for predicting outcome along with the previously investigated ones like muscle atrophy[2] and the duration of symptoms.[10],[19] Of these variables, respiratory dysfunction formed the most sensitive predictor of outcome on logistic regression analysis. The patients with CIM often have a diminished respiratory reserve due to the impaired function either of the phrenic nerves or of the respiratory centres. Damaged lower cranial nerves increase the risk of aspiration pneumonitis.[5] Matsumoto and Symon have reported a mortality in two patients due to sudden respiratory arrest during obex plugging.[21] Williams[5] and Lapras et al[22] have reported patients with CIM who developed a sudden respiratory arrest similar to that seen in our study. Some of these patients probably had the syndrome of afferent respiratory dysfunction, in which normal facilitatory and modulatory feedback pathways were no longer available to make fine adjustments in the respiratory servo mechanisms. Thus, gross responses were handled satisfactorily so that the routine blood gases and vital capacity were deceptively normal and the condition remained undetectable preoperatively but provocative factors like minor trauma, general anesthesia, narcotics and changes in the inspired CO2 mixture caused respiratory deterioration. A number of cumulative factors like laryngeal edema, laryngobronchial secretions, compromise of the diaphragmatic function, weakness of accessory respiratory muscles and increased thoraco-abdominal muscle tone also contribute to the respiratory compromise.[23],[24] The subset of patients with an extremely poor respiratory reserve were identified by their inability to count from 1 to 10 in a single breath and/or to hold their breath for up to 10 seconds.[25] Another sensitive indicator of outcome was the duration of preoperative symptoms [Table - 5b]. A number of patients had a protracted course of the disease. This was supported by the fact that the modified Klekamp and Samii scores[6] did not normalize in these patients despite an adequate posterior decompression. This may be a pointer to an irrevocable injury to the cord leading to neuronal loss; cord ischemia or venous stasis from the compression of vessels lying in a plane perpendicular to the compressing force; persisting syringomyelia; or, to a congenital developmental failure of the brainstem and spinal cord. The aim of surgery in these cases is the stabilization of the clinical manifestations rather than the expectation of significant postoperative recovery.[25],[26] The presence of BI predicted the outcome since it exaggerated the effects of the FM block produced by the tonsillar herniation pressurizing the respiratory centre, bulbar nuclei and long tract.[27] The posterior decompression occasionally exaggerates the cervico-medullary kink produced by BI due to the removal of the posterior bony support, leading to further neurological deterioration. Perhaps, simultaneous transoral decompression with posterior decompression and stabilization, as advocated by Menezes et al, would be more appropriate for these patients.[3] Various authors have described meningeal fibrosis or dural bands associated with CIM and syringomyelia.[4],[5] Although a high association of dural bands with CIM and syringomyelia was also seen in the present series, our statistical analysis revealed that it was not a significant predictor of outcome. Some studies have emphasized the role of tonsillar descent in influencing outcome and have advocated tonsillar resection along with posterior decompression.[23] We did not find any association between the extent of tonsillar descent and outcome. In these cases, symptoms possibly appear due to the gradual development of arachnoidal adhesions near the FM, secondary to trauma caused by the tonsillar motion with repeated Valsalva maneuvers.[3] Therefore, the clinical outcome following surgery is independent of the extent of tonsillar descent. ACKNOWLEDGEMENTS The authors are grateful to Dr. Uttam Singh, Assistant Professor, Department of Biostatistics, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India for his help with the statistical analysis in this study. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04158t1.jpg] [ni04158t3.jpg] [ni04158t5b.jpg] [ni04158t5a.jpg] [ni04158t4.jpg] [ni04158t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}