 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 475-477 Original Article Chronic subdural hematoma: Results of a homogeneous series of 159 patients operated on by residents Gastone Pansini, Fabrizia Cioffi, Homere Mouchaty,
Francesco Cacciola, Alberto Maleci, Nicola Di Neurosurgical Clinic, University
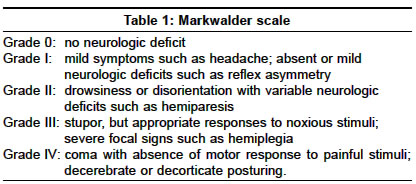
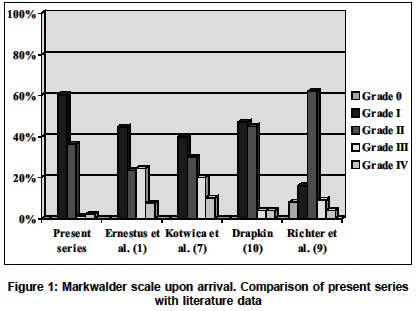
of Florence Code Number: ni04159 ABSTRACT AIMS: A series of cases with chronic subdural hematoma operated upon by residents in neurosurgery is analysed.MATERIALS AND METHODS: 159 patients treated between 1998 and 2001 were included in the study. Mean age was 76.4 years and male/female ratio was 1.7/1. The patients were classified both on admission and at discharge according to the Markwalder scale. The standard operative procedure consisted of an enlarged single burr-hole, rinsing the subdural space with iso-osmotic saline solution and insertion of a subdural drain. CONCLUSION: In CSDH, operation by the residents is safe and the results are comparable to those of the major series of the literature as the surgical procedure is standardized. Key Words: Chronic subdural hematoma, surgical training, head injury. INTRODUCTION The surgical procedure for chronic subdural hematoma (CSDH) is standardized and usually is one of the first operations performed by the neurosurgery residents.[1],[2],[3],[4] At our department, beginning from 1998, the performance of this operation has been entrusted to the residents from the second year of training onwards. In the literature only Mellergard and Wisten[4] made a comparison with regards to the number of recurrences in the CSDH treated by staff neurosurgeons and those by neurosurgeons in training. The aim of the presented study is to evaluate if the results of surgery obtained in our patients are comparable to the major series in the literature in terms of outcome, recurrences and mortality. MATERIALS AND METHODS From January 1998 to December 2001, 159 patients were surgically treated for CSDH at our department. These cases were analysed retrospectively. 101 were males and 58 females (ratio m/f = 1.7/1). Mean age was 76.4 years and the ages ranged from 29 to 96 years. In all cases diagnosis of CSDH was made by Computed Tomography (CT) scan and in some cases by Magnetic Resonance Imaging (MRI). Neurological assessment on arrival at our institution was performed using the Markwalder scale[5] for CSDH [Table - 1]. The same criterion was subsequently applied for the evaluation of outcome. In 101 patients (64%) head trauma of various degrees of severity was the cause of CSDH, while the cause was undetermined in the remaining 58 (36%). In 48 cases (30%) the hematoma was bilateral. A concomitant systemic disease was identified in 87 patients (55%). There was arterial hypertension in 56 (36%) patients, cardiopathy in 27 patients (17%), psycho-organic syndrome in 18 (11%), diabetes in 17 (11%), obstructive chronic broncopathy in three (2%), chronic renal failure in two cases (1%) and haematological discrasies (polycythemia vera and monoclonal gammopathy) in two cases (1%). Associated risk factors were treatment with anticoagulant drugs in 19 patients (12%), with antiaggregant drugs in 19 cases (12%) and chronic alcoholism in 3 cases (2%). At the moment of hospitalization, the clinical grading of each patient was done according to the Markwalder scale. 84 patients were grade I (53%), 64 were grade II (40%), five were grade II (3%) and six patients were grade IV (4%). The residents in the second year of their training performed surgery in each case under the supervision of a staff neurosurgeon. Bilateral hematomas were treated in the same setting. In 95 cases (60%) surgery was carried out in local anaesthesia and in general anaesthesia in the remaining 64 (40%). The surgical procedure was standardized for all patients: after a skin incision of approximately eight cm, a burr-hole was placed over the thickest portion of the hematoma and subsequently enlarged up to a diameter of approximately three cm. The dura mater was incised in a cross-shaped fashion and after coagulation of the dural borders; the external capsule of the hematoma was coagulated and incised, leading to evacuation of fluid material. Irrigation with normal saline at 37 °C was then performed until a clear reflux was obtained. In 44 cases (28%) the internal capsule of the haematoma was sharply fissured because of underlying fluid collection while in 115 cases (72%) it was left untouched. In all cases a 7 mm flat drainage tube was positioned in the sub-dural space, exteriorized through a separate stab wound and connected to a closed drainage system under very gently suction. The drainage was left in place for 48-72 hours. Patients in good clinical condition, i.e. grade 0-I Markwalder scale, were allowed to walk around in the hospital as soon as they were able to, while the remaining patients were kept in the supine position with the head of the bed elevated at 30 degrees. This position according to the prospective randomized study of Nakajima[6] is not a risk factor for recurrence. The patients did not receive any specific medication such as steroids, anticonvulsants or hyperhydratation. RESULTS Five patients (3%) of this series died in the peri-operative period. Three of these patients were older than 85 years and one was a chronic alcoholic. In four cases death occurred after the first procedure. One patient having polycythaemia, died after a second surgical procedure carried out after a three month period as he developed a fresh subdural haematomas. 112 patients (73%) were discharged within seven days and 42 patients (27%) were discharged to home or to a nursing home within three weeks of surgery. There were post-operative complications in seven cases (4%). Four patients (high grades of Markwalder scale) suffered episodes of dyspnoea caused by bronchopneumonia and airway secretion accumulation. The symptom in each case resolved with appropriate antibiotic therapy. Two patients had partial motor seizures, which were managed successfully with anticonvulsant drugs. One patient had a minor pulmonary embolism. Minor complications such as deep venous thrombosis and urinary infection were seen in some cases. In 10 cases (6.3%) there was a recurrence of CSDH on the same side within three months of surgery. Eight of these patients were older than 75 years, one of them receiving anticoagulant therapy and another two receiving antiaggregant therapy. We did not register any case of further recurrence (re-recurrence). The clinical picture at discharge was evaluated according to the Markwalder scale: 130 patients (84%) were grade 0, 19 patients (12%) grade I, two patients (1%) grade II, two patients (1%) grade III and one patient (1%) grade IV. DISCUSSION The choice of entrusting the operation for CSDH to residents is probably due to the fact that the surgical procedure is relatively straight-forward and the procedure is standardized.[1],[2],[3],[8] The performance of this operation by the residents is not specified in any of the major series except for Mellergärd and Wisten[4], where a comparison is made, with regards to the number of recurrences, between staff neurosurgeons with 4-10 years of working experience and neurosurgeons in training (6 months to 3 years of neurosurgical experience). Mellergärd and Wisten[4] reported better results in patients treated by residents with less than three years of experience. According to these authors, this is due to the fact that a young neurosurgeon applies meticulous attention even while carrying out a relatively "simple" procedure like an enlarged burr-hole for CSDH. We compared the data of our series with eight series reported in the literature, selected on the number of cases treated and the parameters used for evaluation of the patients, in concordance with those chosen by us.[1],[7],[8],[9],[10],[11],[12],[13] Our comparative analysis with the series of Ernestus et al[1], Sambasivan et al[12] and Hamilton et al,[11] only took into account the subgroup of patients treated by simple burr hole and excluded those treated other techniques. The following aspects were examined: mean age, concomitant pathology and risk factors, etiology, neurological picture of the patient on arrival and at discharge, outcome, recurrences and mortality. The statistical comparison was carried out with the C2 test, with 1 degree of freedom and the Yates correction. Statistical significance was established at P<0.01 (1%). Mean age of our patients was higher, with an average of 76.4 versus 63 years in the other series.[1],[7],[8],[9],[10],[11],[12],[13] Concomitant systemic illnesses were higher in number in our series. Trauma as the cause of CSDH was in 2/3 of our cases and in other reported sereis.[1],[7],[8],[9],[10],[11],[12],[13] Neurological picture, upon arrival as well as at discharge, was evaluated with the Markwalder scale. Comparative analysis was performed with the data of Ernestus et al[1], Kotwica et al[7], Drapkin[10] and Richter et al[9], who adopted the same method of evaluation [Figure - 1], [Figure - 2]. The outcome at the time of discharge from hospital was better in our series as 84% and 12% of the patients were classified grade 0 and I respectively. This is in comparison to the average incidence of grade 0 and I of 46.4% and 29.4% respectively as reported in the literature.[1],[9],[10] The difference is statistical significant with P<0.01 (P=91.2 with 1 degree of freedom, for grade 0 at discharge and P=21 with 1 degree of freedom, for grade I at discharge). The incidence of patients discharged with higher grades is similar to the results in the literature [Figure - 2].[1],[9],[10] The number of recurrences in our series (6.3%) equals those of the other authors, even though this percentage varies in the literature from 2.3% (Kotwica et al[7] on 131 cases) to 18.3% (Sambasivan et al[12] on 60 patients) with an average of 6.6%.[1],[7],[8],[9],[10],[11],[12],[13],[14] The difference between our recurrence rate and the literature is not statistical significant with P<0.01 (P=0.03 with 1 degree of freedom). Mortality was 3% in our series, in comparison to 2.7% mortality reported in the literature.[1],[7],[8],[9],[10],[11],[12],[13],[14] The difference is not statistical significant with P<0.01 (P=0.34 with 1 degree of freedom). REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04159t1.jpg] [ni04159f2.jpg] [ni04159f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}