 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
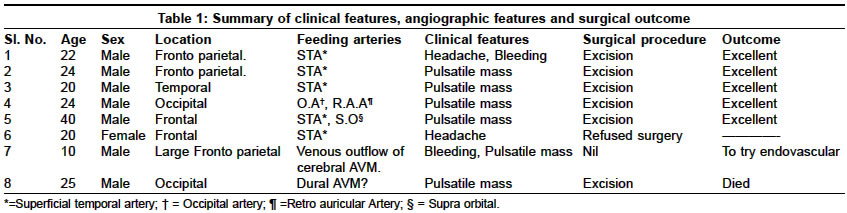
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 478-481 Original Article Scalp arteriovenous malformations Shenoy SatyanarayanaN, Raja A Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal Code Number: ni04160 ABSTRACT
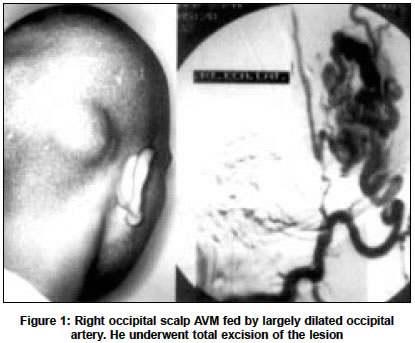
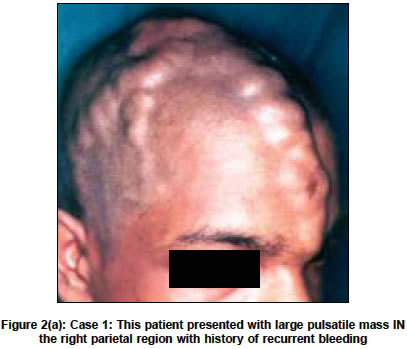
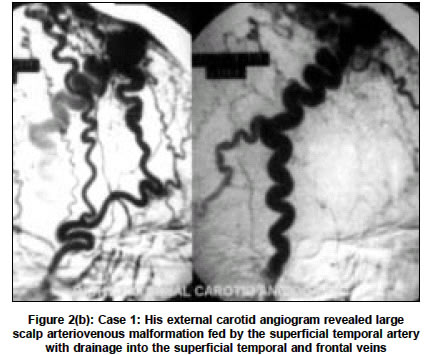
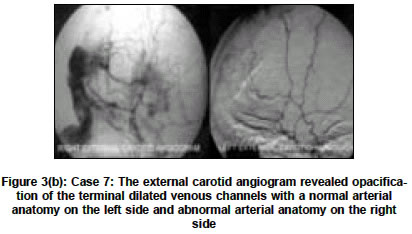
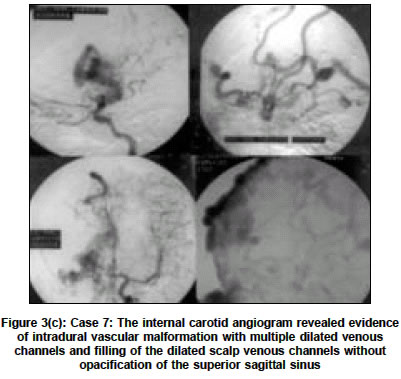
AIMS: We discuss our experience with the surgical management of scalp vascular malformation and review the literature on the subject. Key Words: Scalp, arteriovenous malformation, cirsoid aneurysm INTRODUCTION Arteriovenous malformations (AVM) of the scalp are relatively rare vascular lesions present as an innocuous looking subcutaneous scalp lump or a large, grotesque, pulsatile mass with a propensity to massive hemorrhage.[1],[2] Depending upon the origin of the feeding arteries, we classified scalp malformations into two groups: Group I-primary scalp vascular malformations and Group II-secondary scalp venous dilatations. Various treatment options that have been adopted to treat these lesions include: surgical excision,[1],[3],[4],[5] ligation of feeding vessels, transarterial and transvenous embolization,[4],[6],[7] injection of sclerosant into the nidus[8],[9] and electro thrombosis.[10],[11] In this article we describe the clinical features and discuss the results of the surgical management of scalp vascular malformations. MATERIAL AND METHODS Eight patients, seven males and one female with a mean age of 23 years, were admitted to our hospital in the last six years from 1997 to 2002 with a pulsatile mass on the head [Figure - 1]. Three patients had a history of trauma to the head and two each presented with a history of headache and recurrent bleeding. In all the patients, bruit and thrill was present over the swelling. All the patients were investigated with selective internal and external carotid angiography to determine the feeding vessels, define the anatomical extent of the lesion and to isolate the intracranial component of the malformation. Depending on the angiographic features, we have classified the scalp AVM into two different categories: Group I: primary scalp arteriovenous malformations and Group II: secondary venous dilatations. In the primary scalp vascular malformations, the feeding vessels originate from the calvarial branches of the external carotid arteries, ophthalmic arteries and vertebral arteries and the venous drainage is into the scalp venous system. In Group II, the dilated channels are the main outflow vessels of the intracranial vascular malformations. Six patients belonged to Group I and two patients to Group II. The patient age, location, primary arterial supply of the fistula, treatment and outcome are summarized in [Table - 1]. Operative technique The patient was positioned with the head elevated 20-30 degrees above the heart level for adequate venous drainage. The scalp flap was devised depending upon the anatomy of the nidus of the vascular malformation and the direction of the feeding vessels. While planning the scalp flap, the feeding scalp vessel was preserved in the base of the flap and the flap incorporated one or more normal non-feeding vessels to safeguard the vascularity of the scalp. The skin incision is infiltrated adequately with lignocaine with adrenaline 1:100000 strength, taking care to avoid entering into the dilated venous channel. The scalp is incised in short segments with careful hemostasis using Cushing′s hemostatic forceps. The scalp flap is raised along with the pericranium. The bleeding from the bone is controlled with bone wax and monopolar diathermy. The feeding arteries are identified along their course at the base of the scalp flap, and the pericranium and galea incised, and the vessels traced distally towards the nidus of the scalp malformations and ligated and divided. As the feeding vessels are ligated, the vascular malformation is devascularized. The pericranium and the galea are circumferentially incised and the vascular malformation is excised. RESULTS Five patients in Group I underwent total excision of the lesion successfully without any significant blood loss. In all these patients, the wound healed primarily without necrosis. None of our patients developed recurrence of the lesion during an average follow-up period of 36 months. One patient in Group II (Case 8), had scalp vascular dilatation simulating a primary scalp vascular malformation. Following excision, he developed severe postoperative brain edema and vaso-congestion on the second postoperative day and despite all modalities of therapy he died. Illustrated cases Case 1 This 22-year-old gentleman presented with a large pulsatile mass over the right parietal region with history of recurrent bleeding. A selective external carotid angiogram revealed large dilated, tortuous branches of the superficial temporal artery with enormously dilated superficial temporal and frontal veins. He underwent presurgical transarterial embolization using gelfoam and total excision of the lesion [Figure - 2a and 2b] . Case 7 This 10-year-old boy presented with a large pulsatile mass over the forehead, with history of recurrent massive bleeding. His external carotid angiogram revealed opacification of the terminal dilated venous channels with a normal arterial anatomy on the left side and abnormal arterial anatomy on the right side. However, the internal carotid angiogram revealed evidence of intradural vascular malformation with multiple draining veins and filling of the dilated scalp venous channels. Hence he was diagnosed to have Group II vascular malformation and advised endovascular treatment [Figure - 3a, 3b, 3c] . Case 8 A 25-year-old gentleman presented with history of pulsatile swelling over the occipital region. On examination he had bilateral pulsatile mass in the occipital region. His angiogram revealed tortuous blood vessels in the region of the occipital artery on both sides. He underwent inverted U- shaped scalp flap. The occipital arteries were dissected and ligated. The dilated scalp vascular malformation was dissected. The lesion was pulsatile and bled profusely despite ligation of both occipital arteries. On further dissection, a vascular communication was identified traversing through the bone in the region of the superior nuchal line. Both these connections were divided and the lesion was excised. However, postoperatively the patient developed severe refractory brain edema and progressively worsened and died. DISCUSSION The vascular malformation of the scalp is an abnormal arteriovenous communication situated within the subcutaneous fatty layer of the scalp with the feeding arteries derived from the vessels supplying the scalp. Various names being used to describe the vascular malformations of the scalp include aneurysm cirsoide, aneurysma serpentinum, aneurysm racemosum, plexiform angioma, arteriovenous fistula and arteriovenous malformation.[3],[12],[13] The location of scalp arteriovenous fistulas is roughly evenly distributed among the frontal, temporal and parietal regions.[7] The main sources of blood supply to the scalp are located in the subcutaneous tissue and originates from the external carotid, occipital and supraorbital arteries.[14] The superficial temporal artery is frequently involved in traumatic cirsoid aneurysm due to its long unprotected course.[6] The etiology of these lesions is still controversial. However, it is generally accepted that it may be either of congenital or traumatic origin.[1] About 10 to 20% of scalp arteriovenous malformations develop following penetrating or non-penetrating trauma to the scalp.[12],[13],[15],[16] In this series, three patients had blunt injury to the head. However, these patients noticed the swelling many years later. Most of the patients reported in the literature had a history of progressive increase in the size of the lesion and had become symptomatic in the third decade of life.[3],[13] The clinical manifestations relate primarily to the size of the fistula, and patients may present with loud bruit, hemorrhage, and throbbing headache and in severe cases, scalp necrosis.[6] Hemorrhage from the lesion is uncommon and is usually associated with large vascular malformation. Two patients in this series had bleeding from the lesion; one of the patients had recurrent massive bleeding giving rise to shock. Angiography is the gold standard investigation to delineate the lesion and to exclude an intracranial component.[17] Management of scalp arteriovenous malformation is difficult because of its high shunt flow, complex vascular anatomy and cosmetic problems. The indication of treatment includes cosmetic relief of the pulsatile mass, prevention of hemorrhage and other symptoms such as headache and tinnitus. The treatment options include surgical excision,[1],[2],[3],[4],[5] ligation of feeding vessels, transarterial and transvenous embolization,[4],[6],[7] injection of sclerosant into the nidus[8],[9] and electro thrombosis.[10],[11] Surgical excision is the most common and successful method of dealing with scalp arteriovenous malformation.[1],[3],[13] Various techniques have been used to control the hemorrhage during surgery including percutaneous sutures of the feeding vessels,[3] interlocking suture along the line of incision, and use of tourniquet and intestinal clamp over the base of the flap.[14] A step-wise incision as suggested by other authors with careful pressure control is a useful method to control the scalp bleeding.[1] We reflected the pericranium along with the scalp flap to prevent inadvertent rupture of the nidus. Contrary to some reports, we did not find any significant pericranial component of the malformation.[1] As scalp AVM has a potential to evolve, the anomalous arteriovenous communication must be completely eliminated because recurrence or enlargement is reported after an incomplete treatment.[4],[13] Incomplete treatment can also cause scalp necrosis and bleeding. We have used a wide based scalp flap including uninvolved scalp arteries and ligation of the feeding artery near the nidus to prevent scalp necrosis. Endovascular treatment of scalp arteriovenous malformation can be used as definitive therapy or as an adjunct to surgical therapy in reducing blood loss during excision.[4],[6],[7],[11] Embolization of both feeders and nidus before surgery is safer than embolization of the feeders alone when considering preoperative embolization to reduce the risk of massive hemorrhage.[4] Three different approaches have been used to access the fistula, namely femoral transarterial, femoral transvenous and direct percutaneous catheterization of the feeding arteries or draining veins.[4],[6],[7],[9],[11] Direct percutaneous catheterization of the fistula has been used whenever access through the artery or vein is not possible.[6] The percutaneous placement of thrombogenic coils is a simple and effective method to produce thrombosis of cirsoid aneurysm of the scalp, especially after slowing down the blood flow through transvascular intra-arterial embolization.[11] Recurrence of the lesion has been seen as late as 18 years after complete surgical resection of the malformation.[1],[17] To conclude, even though diagnosis of scalp AVM can be made easily, a complete angiographic study of the lesion has to be performed to differentiate primary scalp vascular malformations from secondary venous dilatations. Primary scalp vascular malformation can be excised completely without significant blood loss and scalp necrosis. However, excision of secondary scalp venous dilatation without treatment of the intracranial component can be life-threatening. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04160t1.jpg] [ni04160f3b.jpg] [ni04160f1.jpg] [ni04160f3a.jpg] [ni04160f2b.jpg] [ni04160f3c.jpg] [ni04160f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}