 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
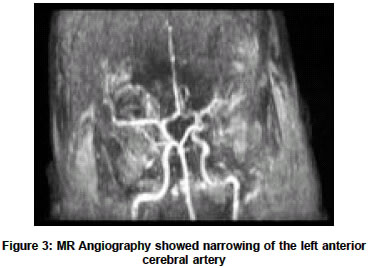
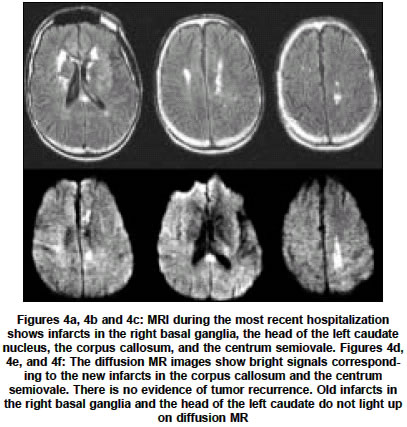
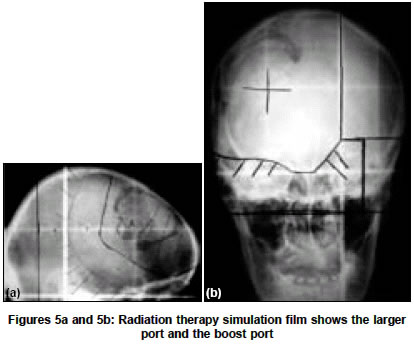
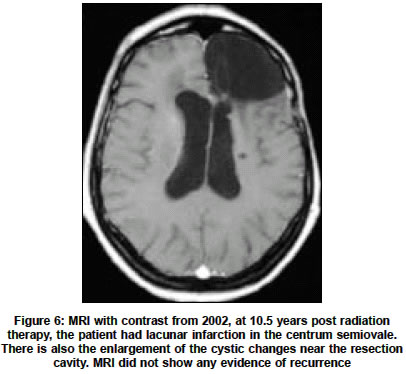
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 482-486 Case Report Accelerated cerebral vasculopathy after radiation therapy to the brain Penagaricano JoseA, Linskey MarkE, Ratanatharathorn Vaneerat Departments of Radiation Oncology and Neurosurgery, University of Arkansas for Medical Sciences, 4301 W. Markham, Little Rock, Arkansas - 72205 Code Number: ni04161 ABSTRACT Brain irradiation is commonly used for many primary brain malignancies. We will present two cases of post-radiation vasculopathy of large arteries of patients who received radiation therapy to the brain as part of their tumor management. We will underscore the significance of this condition and suggest the overall management of patients receiving brain radiation at an early age. Key Words: Vasculopathy, Radiation damage, Brain tumor. INTRODUCTION Central nervous system tumors have the second highest incidence among pediatric malignancies. The 1999 annual incidence in the United States, of CNS tumors in the population age group of 0-20 years old, is 2,200.[15] Brain irradiation has been used as one of the three major modalities of treatment for CNS tumors. As patients live longer, devastating complications may manifest. Some long-term complications of radiation therapy are well known such as toxic encephalopathy and growth and development impairment. Others are lesser known even to radiation oncologists. Radiation-induced vasculopathy of large arteries secondary to brain irradiation is one such complication. These patients irradiated at a young age appear to develop accelerated atherosclerosis and suffer from repeated small strokes at a young age.[1],[2],[9],[12],[14],[16],[17],[18] The intent of our paper is to underscore the significance of this complication and to make some suggestions in the overall management of patients receiving radiation therapy at a young age. Case 1 A 34-year-old white male was diagnosed with unresectable right thalamic low-grade astrocytoma in 1984 treated with whole brain radiation therapy with 4 MeV X-Ray to 54 Gy [Figure - 1] followed by 6 Gy boost, all given at 2 Gy per day using parallel-opposed ports [Figure - 2]. The boost treatment used loading favoring the side of the tumor. The total dose to the tumor was 60 Gy. The patient was doing well for several years with no evidence of recurrence. Approximately 18 years later, the patient presented to the emergency room with history of lower extremity weakness, slurring of speech, and right-left disorientation as noted by the emergency room physician. There were no risk factors for atherosclerosis such as diabetes, hypertension or smoking. The patient was admitted for evaluation and found later to have slowed mentation, right-left disorientation, calculation problems, mild right-sided extremity weakness, moderately increased tone in the lower extremities, severe ataxia including truncal ataxia, clonus, positive Babinski, and brisk deep tendon reflexes throughout. He was unable to walk without assistance. The patient was diagnosed with right-sided subacute stroke. Magnetic resonance angiography (MRA) showed narrowing of the left anterior cerebral artery [Figure - 3]. Magnetic resonance imaging of the brain did not show any evidence of recurrence and clearly demonstrated the temporal sequence of the effect of radiation on small vessels and subsequently on larger arteries. [Figure - 4]a is the T1 pulse sequence MRI that showed areas of infarcts in the right basal ganglia, head of the left caudate nucleus, and the corpus callosum. [Figure - 4] b and c show infarcts in the left centrum semiovale. The infarcts in the right basal ganglia and the head of the left caudate nucleus are secondary to the effect of radiation on the smaller perforating arteries supplying these regions. The diffusion MR images [Figure - 4] d,e,f show bright signals in the corpus callosum, and in the left centrum semiovale consistent with new infarcts following the distribution of the left anterior pericallosal artery. This is consistent with the finding of the narrowing of the left anterior cerebral artery on the MRA. The two areas of old infarcts do not light up on the diffusion MR. The patient was started on aspirin 81 mg per day. He was also placed on fludrocortisone to bolster his blood pressure since his watershed stroke could potentially be worsened by hypotension. His fludrocortisone was adjusted to regulate his blood pressure. His symptoms and signs improved such that only ataxia remained severe. Case 2 A 47-year-old white female was diagnosed with anaplastic astrocytoma beginning in the premotor gyrus of the left frontal lobe in 1992, treated with gross total resection and postoperative radiation therapy. Parallel-opposed (right and left lateral) and right anterior ports with shaped blocks were used. Energy selection was 6, 18, and 6 MeV X-rays, respectively. Patient was given 50.4 Gy at 1.8 Gy per day followed by 9 Gy boost with the right and the left lateral ports to the postoperative volume [Figure - 5] with differential loading favoring the right side. The total dose to the postoperative volume was 59.4 Gy. The patient also received chemotherapy with intra-arterial cis-platinum and systemic methotrexate. Her initial deficit with right-sided weakness and expressive aphasia improved significantly after her surgery to the point where she had near normal verbal output and she could ambulate independently. She did have some cognitive difficulty and her husband was named her power of attorney. She had done well for several years. Nine years post-treatment, the patient slowly developed new right-sided weakness, worsened aphasia and new dysarthria. She then developed urinary incontinence. The patient deteriorated globally and became wheel-chair-bound. She needed help with transfer and bathing. She was unable to do minor hygiene tasks such as washing her face and brushing her teeth without assistance. Her Karnofsky performance status dropped to 50. She also had ongoing seizure with her last clinical seizure occurring a year earlier. There were no risk factors for atherosclerosis such as diabetes, hypertension or smoking. Examination showed she was severely dysarthric. She had obvious expressive aphasia with word substitution error and word-finding difficulties. She was unable to do accurate repetition. Her muscular tone and bulk were largely normal except for slight increased tone on the right side. She also had mild right-sided paresis. Her recent magnetic imaging study showed a large resection cavity extending from the premotor gyrus all the way forward to the frontal lobe. There were no signs of recurrence or persistent disease. There was no mass effect. She had some increased signal on FLAIR and T2-weighted images around the resection cavity most consistent with post-resection gliosis or post-radiation changes. She also had an obvious lacunar infarction present in the left centrum semiovale extending down to the internal capsule [Figure - 6]. The assessment indicated that she probably had toxic encephalopathy from the combined chemotherapy and radiation therapy given 10.5 years earlier, evident as cognitive impairment and urinary incontinence. She also had stroke-like symptoms consisting of the new right-sided weakness related to the lacunar infarction. This second case showed the effect of radiation therapy on smaller vessels of the brain and toxic encephalopathy. DISCUSSION The syndrome of accelerated cerebral vasculopathy after cerebral radiation therapy is poorly recognized in the community of radiation oncology. Vasculopathy, for example, is usually not included in informed consents as a part of the complications of radiation therapy to the brain for pediatric and young adult patients. Nevertheless, radiation-induced vasculopathy reports can be found as early as the 1960s.[6],[7] Toxic encephalopathy is more frequently recognized. Radiation injuries to small vessels and capillaries are well recognized. The vulnerability of small vessels and capillaries to radiation is attributed to the constructs of the small vessels with endothelial cells, the main target of radiation injuries, surrounded by basal membranes.[8] Injuries to small vessels manifest earlier than injuries to large arteries as demonstrated in our two cases. However, the conventional teaching in radiation oncology is such that radiation-induced damage to large arteries is uncommon. Pathological changes seen in these large arteries may include intimal proliferation with or without atheromatosis, thrombosis, and occasional rupture. But, in fact, the clinical significance of radiation-induced vasculopathy is much greater than the recognition it receives. Radiation injuries to carotid arteries were well reported in patients having neck irradiation in which abnormal phonoangiograms were found in 25% of the patients.[4] But radiation-induced vasculopathy after cerebral irradiation in young patients is rarely reported in radiation oncology literature.[2],[9] The diagnosis of radiation-induced vasculopathy, to a great degree, is a diagnosis by exclusion coupled with any relevant history of radiation therapy to the affected vessels. Conditions that predispose patients to vasculopathy have to be ruled out, namely vasculitis, collagen vascular diseases, atherosclerosis, neurofibromatosis, primary moyamoya syndrome, and other causes of occlusive vasculopathy such as compression by tumors, diabetes mellitus, hypertension and so on.[13],[14] Radiation injuries to large vessels may take the form of occlusive vasculopathy or vascular malformation. Epstein et al reported that the neuroradiographic findings of radiation-induced angiomatous changes may appear as mass lesions and may be mistaken for recurrent tumors, leading to inappropriate treatment with antineoplastic agents such as chemotherapy.[5] Epstein et al reported radiation-induced angiomatous malformation in three pediatric patients treated for suprasellar tumors at dose-fractionation regimens that appeared very "safe," i.e. 45- 50.4 Gy at 1.8-2 Gy/ fraction. The pathogenesis of angiomatous changes in irradiated vessels is unclear. However, the two cases we described had occlusive vasculopathy, one (Case 1) took the form of multiple small strokes. These patients, who were irradiated at a young age, appeared to have accelerated atherosclerosis. The dose response relationships as well as volume effect are unclear since most reports lack details of radiation therapy dose and techniques. This is further complicated by the poor recognition of the condition. Most reported cases with radiation-induced vasculopathy received irradiation in the parasellar region. The dose levels reported in the published literature show that a large proportion of these reported radiation-induced vasculopathy cases, in intra- and extracranial sites, were treated with dose-fractionation schemes that were "safe." The lowest dose reported to be associated with injury to large arteries is 10 Gy. On the contrary, Brant-Zawadzki et al suggested that the threshold dose of 50 Gy appeared to exist.[3] This report of dose-response relationship appears to be supported by the report of Grenier and associates, in which the vasculopathy occurred in the posterior cerebral arterial distribution in two patients treated for medulloblastoma with boost to the posterior fossa. Whole brain was treated to 40 Gy in both patients but the posterior fossa was boosted to 55 Gy total cumulative doses.[10] Cases of radiation-induced vasculopathy in the more modern series center around higher dose levels such as 50-60 Gy given at conventional fractionation. Some also received repeated irradiation with cumulative dose levels as high as 90-120 Gy.[1] Therefore, good technique and dose prescription do not totally circumvent radiation-induced vasculopathy. Unfortunately, the authors did not provide the denominator so the incidence is not known. Gamma Knife stereotactic radiosurgery had also been reported to cause radiation-induced vasculopathy. The radiation dose to the large blood vessels in one of the reports, typically internal carotid arteries, was not extremely high but was calculated to be 18 Gy.[1] However, the large dose per fraction inherent to stereotactic radiosurgery may be more injurious to blood vessels and may be the main reason that brought on the vasculopathy. The incidence of radiation-induced vasculopathy for any particular dose-fractionation scheme is not known since almost none of the reports provide denominators. One series mentioned 3 patients with radiation-induced occlusive vasculopathy of large arteries after radiation therapy for germ cell tumor of the central nervous system in 105 patients.[19] Another series reported 3 out of 139 patients irradiated for pituitary adenoma, to 40-60 Gy, with cerebral ischemic events thought to be caused by radiation therapy, occurring at 5-7 years post radiation therapy.[11] There is a small number of cases reported in the published literature, mostly young patients irradiated to the vicinity of the sellar region. There is also a report of the preponderance for the occlusion to occur in the supraclinoid portion of the internal carotid artery. Different radiation types had been implicated as the cause of the vasculopathy including fractionated external beam radiation therapy, Gamma Knife stereotactic radiosurgery, and colloidal gold intracystic instillation. Nevertheless, it appears that no part of the brain is exempt from this type of complication. The latency from the treatment to the development of vasculopathy ranges widely from 2 to 25 years. However, the vast majority of patients who ultimately ended up with vasculopathy manifested their first symptoms in less than ten years after the treatment.[1] Although the latency period is long, the symptoms, once they appear, are not infrequently acute. Transitory improvement may occur but most frequently, slow deterioration is seen. Patients usually present or develop stroke-like symptoms as seen in our case reports. The deterioration tends to be global and may involve motor function, sensory loss, ataxia, speech difficulty, or decreased cognitive ability. These transient ischemic episodes tend to occur repeatedly resulting in progressive and slow global deterioration in the patients′ functional status. The second most common presentation is seizures.[13] Montanera et al reported the coexistence of a radiation-induced meningioma and vasculopathy.[13] They cautioned that vascular supply to the tumor as well as to the remainder of the brain be carefully studied in patients with prior brain irradiation. Transdural collateral vascularization may be the main source of blood supply to the rest of the brain in patients who may also have vasculopathy. It is crucial that these anastomoses be preserved at the operation. Magnetic resonance imaging of these patients prior to radiation therapy serves as baseline documentation of the patency of blood vessels prior to treatment. The post-radiation MR picture is similar to what one would see in atherosclerosis. Wall thickening and prominent enhancement is seen on MR even several years after the occurrence of occlusion or stenosis. Multiple areas of infarcts can be seen following arterial distribution of the affected vessels. The two cases reported here are both severely debilitated. One case was treated with radiation therapy only but the volume was whole brain to 54 Gy followed by boost to total of 60 Gy. The second case was treated by radiation therapy to a much smaller volume but the patient had large surgical resection, chemotherapy and radiation therapy to 59.4 Gy. These two cases underscore the importance of the irradiated volume, and the cumulative toxicities from multimodality therapy. In the era of multimodality image-guided radiation treatment planning (3-dimensional conformal therapy and intensity-modulated radiation therapy) large arteries that need not be included within the treatment field can be intentionally spared. The large arteries can be easily visualized on contrast MR studies and on MR angiography. Clear delineation of tumors and critical structures is useful in planning 3-dimensional radiation therapy and intensity-modulated radiation therapy (IMRT). In the latter technique, all target and critical structures will need to be outlined and entered as objectives and constraints respectively to allow conformal coverage and conformal avoidance. Thus far, we do not know how we can circumvent or even decrease the chance of radiation-induced vasculopathy. It does not appear that the adjustment of time-dose-fractionation and volume is reliable in circumventing this complication. Early corticosteroid administration prior to and throughout the course of radiation therapy has been suggested as prophylaxis. But its efficacy remains unproven. Treatment with baby aspirin has been reported to be helpful and may reverse some of the symptoms. The best method remains prevention by delaying radiation therapy in young patients as much and as long as possible. If treatment is needed, then modern planning technique and delivery with conformal coverage and conformal avoidance can be used as the preventive method to circumvent radiation-induced vasculopathy. It is also unclear how much systemic chemotherapy contributes to the development and the severity of vasculopathy. The patient in Case 1 did not receive any chemotherapy as part of his tumor treatment. This patient received radiation using standard fractionation of 2 Gy per fraction to the whole brain. The treatment volume of whole brain is unusual for a low-grade astrocytoma. We believe that this patient represents a true case of radiation-induced vasculopathy with reference to the dose and volume of radiation utilized to manage his tumor. In addition, the presentation of symptoms correlates with the latency period for this condition. The follow-up of long-term survivors will need to keep possible vasculopathy in consideration as well as toxic encephalopathy. Neuro-imaging studies are helpful in detecting vessel changes, which may alert clinicians toward the possibility of the development of vasculopathy so potential therapeutic measures may be considered at that time. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04161f3.jpg] [ni04161f2.jpg] [ni04161f5.jpg] [ni04161f4.jpg] [ni04161f6.jpg] [ni04161f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}