 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
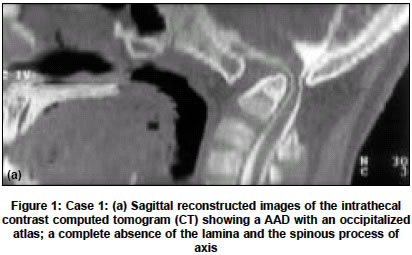
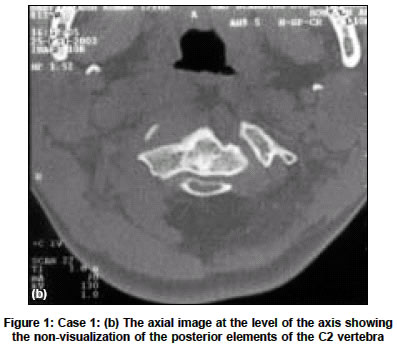
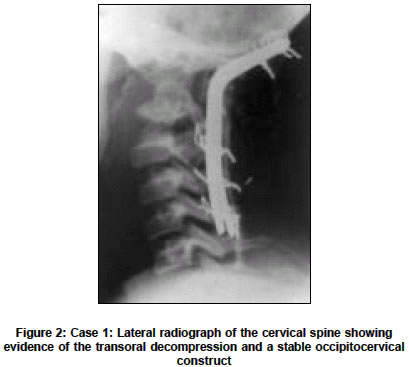
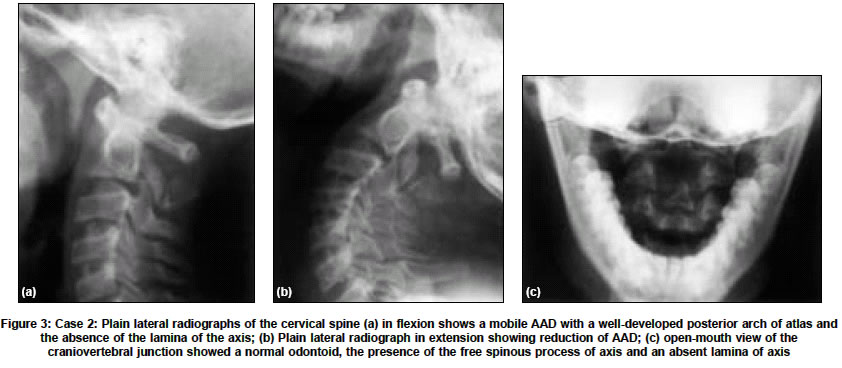
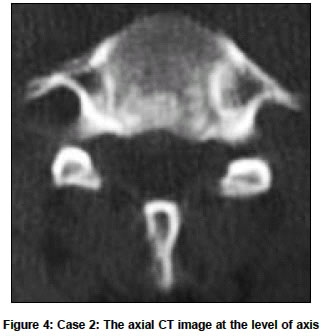
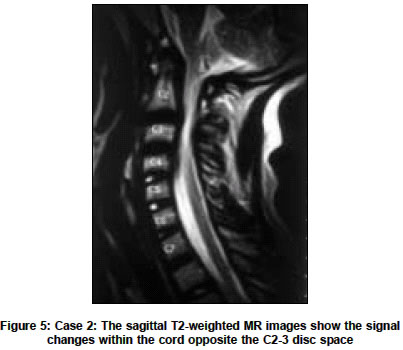
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 489-491 Case Report Atlantoaxial dislocation associated with the maldevelopment of the posterior neural arch of axis causing compressive myelopathy Behari Sanjay, Kiran Kumar MV, Banerji Deepu, Chhabra DevendraK, Jain VijendraK Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow - 226014 Code Number: ni04163 ABSTRACT The craniovertebral junction has a predilection for a variety of congenital anomalies due to its complex development. The association of atlantoaxial dislocation (AAD) with the maldevelopment of the posterior arch of axis is extremely rare. We report two such cases and present the management strategy.Key Words: craniovertebral anomalies, atlas, axis, spine fusion, atlantoaxial dislocation, anomalies of axis INTRODUCTION The complex development of the craniovertebral junction makes it prone to a myriad of congenital anomalies. There are a few case reports of the rare anomalies of the posterior neural arch of the axis.[1]-[4] Absence of the posterior elements of the axis have been associated with instability at the C2-3 level; 3 its association with atlantoaxial dislocation, however, has not been previously reported.[3] In the present study, we report two such cases and analyze the embryological basis for the maldevelopment of the posterior elements of the axis and its association with AAD. CASE REPORT Case 1 A 12-year-old boy presented with neck pain, restricted neck movements, paresthesia of all the limbs and progressive spastic quadriparesis for 7 months. There was no history of trauma or an associated inflammatory or connective tissue disorder. Lateral radiographs of the craniovertebral junction in flexion and extension, sagittal and axial reconstructed images of the intrathecal contrast computed tomogram [Figure - 1a, 1b] showed a fixed AAD with an occipitalized atlas and a complete absence of the lamina and the spinous process of axis. After the application of Crutchfield′s cervical traction, transoral decompression of the odontoid process and an occipitocervical posterior fusion utilizing Ransford′s contoured rod[7] and onlay rib grafts were performed. At follow-up after 6 months, the patient had a normal power and a significant relief in his spasticity and paresthesia. Lateral radiograph of the cervical spine revealed a stable occipitocervical construct [Figure - 2]. Case 2 A 16-year-old boy, following a trivial trauma to the nape of neck 2 years ago, developed progressive spastic quadriparesis; paresthesia below the level of the neck; and Lhermitte′s phenomenon. Three months prior to admission, he developed urinary urgency, precipitancy and constipation, and difficulty in respiration. There was no history of consanguinity or teratogenic events in utero. His neurological examination revealed a spastic Grade 4 quadriparesis with posterior column impairment but no spinothalamic tract involvement. There was no restriction of neck movements or neck spasm. The clinical, biochemical and radiological examination revealed no evidence of rheumatoid arthritis or any other inflammatory or connective tissue disorder. Investigations revealed a mobile AAD with a well-developed posterior arch of atlas and the absence of the lamina of the axis. The spinous process appeared to be ′free floating′ [Figure - 3], [Figure - 4], [Figure - 5]. The posterior arch of the atlas was well formed except for a small bony segment that was deficient at its junction with the lateral mass on the left side. There was evidence of cord compression opposite the C2-3 disc space. The patient was operated in the prone position with his head resting on a horse-shoe headrest and his neck stabilized utilizing a Crutchfield′s cervical traction. The maldeveloped C2 spinous process and the fibrous bands attaching it to the pedicles were excised to relieve the posterior thecal compression. After ensuring the adequate reduction of AAD, utilizing an intraoperative X-ray image intensifier, the Ransford′s contoured rod[7] and onlay autologous rib graft fusion (that included the occipital bone, the posterior arch of atlas, the laminae of C3 and C4) with sublaminar wires was performed. The patient had an uneventful postoperative recovery. At follow-up after 6 months, he showed near normal power and a marked improvement in spasticity and paresthesia. His respiratory and sphincteric dysfunction as well as the Lhermitte′s phenomenon had also improved. However, he developed mild restriction of his neck movements. The lateral radiograph of the cervical spine at follow-up revealed the reduction of the AAD with a stable occipito-cervical rod and bone graft construct in situ. DISCUSSION The axis develops from the second spinal sclerotome in three essential stages.[1],[8] In the precartilage stage, the cells of the sclerotome migrate ventromedially to surround the notochord forming the centrum that develops into the body. At Stage 23 of embryogenesis (the eighth post-ovulatory week), the cells extend ventrolaterally to form the transverse process and foramen transversarium;[9] and, dorsally to form the neural arch from which the pedicles, articular processes and lamina develop. The chondrification stage of the posterior arch begins at the pedicle during the sixth week of embryogenesis and ends in the midline during the fourth month. The ossification stage extends into the cartilaginous arch by the third to the fourth years of age. The defect in the posterior elements of the axis may be caused by the failure of the extension of the chondrification centers in the posterior arch or by the failure of the ossification process.[1],[8] The complete agenesis of the posterior elements of the axis, as seen in Case 1, implies a very early fault in embryogenesis. In the reported cases of complete agenesis of the posterior elements of the axis, a mobile C2-3 dislocation was present that resulted in a chronically unstable spine.[3],[6] In two of these patients reported by Goel et al,[3] a transoral resection of the compressing elements of the C2 and C3 bodies and the intervening C2-3 intervertebral disc, and posterior stabilization using a multiholed stainless steel plate and wire fixation, was performed. In the case reported by Trivedi et al,[6] relief from the neck pain and C2-3 instability were obtained by a posterior occipitocervical contoured rod fusion with onlay bone graft similar to the technique used in the present case. The presence of an incomplete, congenital absence of the posterior elements of the axis (that was designated as a "spina bifida" of the C2 vertebra), has been reported.[1],[2],[4],[5] These cases perhaps represent a more delayed disorder of embryogenesis in which either partial chondrification or incomplete ossification has taken place.[1],[3] The presence of the remnant of the spinous process of the axis attached to the pedicles by fibrous bands in the present case placed our second patient in this category. Since these maldeveloped posterior elements of the axis were causing thecal compression, their resection resulted in neurological recovery. Asakawa et al,[1] and Koyama et al,[4] have also reported spinal stenosis at the level of C2 vertebra due to the invagination of the bifid lamina of the axis. In both these cases, the resection of the compressing bone and the fibrous bands resulted in neurological recovery.[1],[4] The possible cause of the simultaneous presence of the C1-2 instability could have been laxity of the craniocervical supporting ligaments. The instability could also be due to the presence of incompetent C1-2 lateral joints associated with the disorders of chondrification and ossification of the posterior neural arch of axis.[1],[8] The myelopathic manifestations were due to the thecal compression by the posteriorly dislocated odontoid in the first case; and, the C2 spinous process and the attached fibrous bands from the posterior aspect in the second case. During surgery, stainless-steel contoured rod was fixed to the occipital bone and the subaxial spines utilizing sublaminar wires; an adequate decortication of the occipito-cervical bones was performed; and, onlay, autologous, split rib-bone grafts were placed at the level of the construct, thus fixing the joints above and below the levels of dislocation.[7],[10] Since the occipito-atlantal and atlanto-axial joints contribute significantly to the flexion-extension and rotatory movements at the neck, this reduction and stability were achieved at the cost of restriction of the patient′s neck movements that was only partially compensated by the movements of the lower cervical spine. The effectiveness of the surgical procedure was established by the rapid neurological recovery of the patients. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04163f3.jpg] [ni04163f1a.jpg] [ni04163f1b.jpg] [ni04163f5.jpg] [ni04163f4.jpg] [ni04163f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}