 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
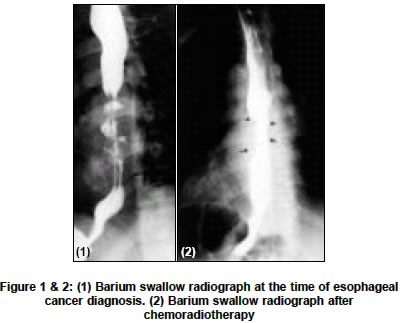
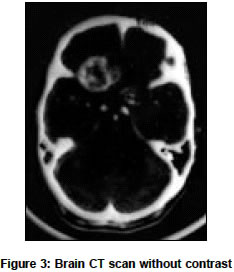
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 492-493 Case Report Brain metastasis from esophageal carcinoma Almasi Saeid, Bashashati Mohammad, Rezaei Nima, Markazi-Moghaddam Nader Radiotherapy Department of Besat Nehaja Hospital, Tehran Code Number: ni04164 ABSTRACT Brain metastasis from esophageal carcinoma is rare. In our center, among 301 cases of esophageal cancer referred for radiotherapy during a 14-year period, brain metastasis from esophageal carcinoma was detected in one case. An unusual case of esophageal carcinoma that presented with brain metastasis is reported.Key Words: Esophagus, cancer, metastasis. INTRODUCTION Brain metastasis from primary neoplasms, such as lung cancer, breast cancer, melanoma, and leukemia is relatively common[1] but metastasis from esophageal carcinoma is rare.[1],[2],[3],[4] Recently, advances in neuroimaging and the increased survival of these patients have led to more frequent and earlier detection of brain metastasis. With these advances, clinical reports of brain metastasis from esophageal carcinoma have increased gradually.[5],[6],[7],[8] In Besat Hospital (Tehran, Iran), among 301 cases of esophageal cancer referred for radiotherapy during a 14-year period (1990-2003), brain metastasis has been detected in only one case. We describe herein this case. CASE REPORT A 52-year-old man was subjected to chemo-radiotherapy, due to an esophageal carcinoma in September 2002. He had presented with history of progressive dysphagia for one year. Investigations revealed an esophageal mass [Figure - 1] and a squamous cell carcinoma was confirmed by pathologic study of endoscope-guided biopsy. External radiotherapy to anterior and posterior aspects of the neck and mediastinum was given. A tumor dose of 5000 cGy in 20-fractions was delivered by linear accelerator 6 Mev units over a two-month period. Also, seven doses of chemotherapy with cisplatin (80 mg) and methotroxate (60 mg) was given during a seven-month period. After the radiotherapy and chemotherapy courses, barium swallow radiograph showed small diverticula at the mid-zone of the esophagus with minimal irregularity at this area. No stricture was seen and deglutition phenomena were normal [Figure - 2]. The patient complained of severe and progressively increasing headache in the frontal area in June 2003, approximately nine months after the diagnosis of esophageal cancer was made. The patient′s performance status was diminished. There were no signs of other organ (liver, lungs and bones) involvement. In the physical examination, a 9-kilogram weight loss from the first visit was detected. In the left supraclavicular area a 5 x 5 cm firm mass, attached to the surrounding tissues was detected, suggesting lymph node metastasis. The chest expansion was limited and the respiratory sounds were decreased suggesting the presence of mediastinal widening. There was no other positive finding in the systemic examination. CT scan of the brain demonstrated a lobulated mass lesion of the left frontal lobe with severe surrounding edema and collapse of the ipsilateral ventricular system [Figure - 3]. Brain metastasis from esophageal carcinoma was clinically diagnosed as per the CT scan findings, and no biopsy was taken for pathologic confirmation. The chest X-ray did not reveal any mass lesion in the lungs. Two opposite field palliative whole brain radiotherapy with the tumor dose of 4000 cGy was delivered in 16-fractions over a 3-week period. The patient did not come to our hospital for further follow-up and he expired with severe respiratory distress 3 months later. DISCUSSION Most recent reports have indicated that the incidence of brain metastasis from esophageal carcinoma has been approximately 1.5%.[5],[6] In general, brain metastasis originates in the lung from either a primary or a secondary lung neoplasm. However, patients with brain metastasis from esophageal carcinoma commonly have no lung metastasis and the most recent reports have indicated that only 15-30% of patients had lung metastasis at the time of diagnosis of brain metastasis.[5],[6] One of the reasons for this may be that the lung metastases are too small to be identified radiologically. Another reason may be a possible pathway through the vertebral venous system (Batson′s plexus).[9] The most common histology in both primary tumor and brain metastasis was adenocarcinoma in the United States,[5],[8] while the most common histology in our country and Japan was squamous cell carcinoma.[6],[10] Therefore, it is not possible to conclude from these data that histology, in itself, is a risk factor for brain metastasis.[5] Although large primary tumors have been indicated as a risk factor,[6],[8] this data was unavailable in our case. Most of the reports have indicated that esophageal cancer patients who developed brain metastasis, in general, have poor prognosis (median survival ranged from 3.6 to 3.9 months).[5],[6],[7] Recent reports have indicated that longer survival of patients with single brain metastasis from esophageal carcinoma (9.6 months) was observed with surgical resection and whole brain radiotherapy.[5] In selected patients who may benefit from effective local tumor control in the brain, such multimodal treatment may provide better results.[5],[6],[7] REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04164f1-2.jpg] [ni04164f3.jpg] |
| |||||||||

{kind=link}
{kind=link}