 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
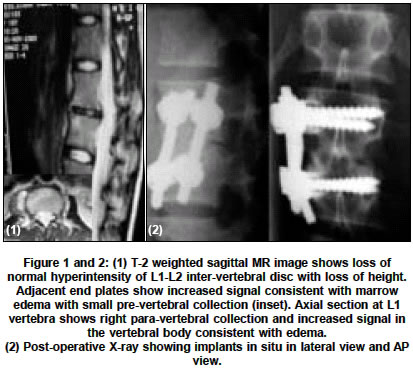
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 499-500 Case Report Salmonella spinal osteomyelitis: A case report and review of literature Acharya Shankar, Bhatnagar Pallav Sir Ganga Ram Hospital, Rajender Nagar, New Delhi - 110060 Code Number: ni04167 ABSTRACT A case of vertebral osteomyelitis is presented where initial presumptive diagnosis of tuberculous infection was made on clinico-radiological grounds but eventually turned out to be Salmonella infection upon exploration, biopsy and culture. Patient recovered completely following debridement and appropriate antibiotics (fluoro-quinolones) for a period of six weeks. Internal fixation allowed early ambulation.Key Words: Salmonella, spinal, osteomyelitis. INTRODUCTION Tubercular infection of the spine in the Indian sub-continent is common. Clinical features, radiological and MR findings are usually enough to establish diagnosis of tuberculosis, though positive confirmation requires tissue diagnosis and culture,[¹][²] Infection of a spinal segment with para-vertebral abscess can prove to be a difficult diagnostic problem.[2] The rising incidence of multi drug resistant tuberculosis has further compounded the issue. Here we present a case of Salmonella vertebral osteomyelitis where a presumptive diagnosis of multi drug resistant tuberculosis was made and surgery performed. CASE REPORT An 18 year old female presented with complaints of backache associated with low grade fever for two months and inability to stand for one month, progressive loss of appetite and weight. She was put on 4 drug anti-tubercular regime on basis of CT report. However the symptoms progressively worsened over next 4 weeks. On presentation to us she was in acute pain, a febrile and normotensive. There was no hepato-splenomegaly. Local examination of the spine revealed that para-vertebral muscles were in spasm and lumbar lordosis was obliterated tenderness over spinous process of L1 and L2, no obvious swelling, no motor or sensory deficit. Her haemogram, urinalysis, blood culture for aerobic and anaerobic bacteria which was negative ESR was 50 mm in 1st hour. MRI study [Figure - 1] showed destruction of L1-L2 disc and involvement of para-discal regions of L1 and L2 with para-vertebral collection at the same level. Presuming it to be a case of resistant tuberculosis, anterior debridement, autogenous bone grafting and stabilization with double rod and pedicle screw system in vertebral bodies [Figure - 2] was performed. Per-operative findings were consistent with tuberculous pathology. However to our surprise, histo-pathology and microbiology reported Salmonella typhimurium from the surgical specimen. Post-operatively a search was made for predisposing condition but tests were negative for any hemoglobinopathy. Blood cultures were negative and serum agglutinins were found to be normal. She was started on injectible fluoroquinolones (Ciprofloxacin 200 mg per 100 ml i.v. twice daily) as per the sensitivity report for two weeks followed by discharge from hospital on oral ciprofloxacin 500 mg twice a day for a total of 8 weeks. She was ambulated on custom made spinal orthosis while still in hospital as the pain subsided DISCUSSION Salmonella, in patients with sickle cell disease is the most common causes of osteomyelitis (70%).[3] However in patients not suffering from sickle cell disease, it accounts for only 0.5% of all cases of osteomyelitis,[4] and involvement of spine is approximately quarter of all these cases.[5] Salmonella typhimurium and S enteritides are the common serotypes involved,[4] and it occurs by hematogenous spread. It shares several features similar to those of pyogenic vertebral osteomyelitis due to other causes,[6] e.g. the bi-modal age distribution, male preponderance, predominantly lumbar involvement and mostly mono-microbial nature of infection. The clinical features of Salmonella infection are usually acute in onset with high fever, chills, severe bone pains, leucocytosis and raised ESR,[7] however they may have insidious onset. Hence the clinician treating vertebral infection should have high index of suspicion to diagnose Salmonella as the infecting agent.[8] The definitive diagnosis of Salmonella vertebral osteomyelitis depends on isolation of organism from the bony specimen or para-vertebral collection,[8] In the Indian subcontinent since tuberculosis is the commonest, lot of clinicians start Empirical treatment of TB on basis of MRI report. We feel minimal invasive techniques like CT guided Fine needle Aspiration or percutaneous transpedicular Craig biopsy needles can be used to obtain tissue diagnosis. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04167f1-2.jpg] |
| |||||||||

{kind=link}