 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
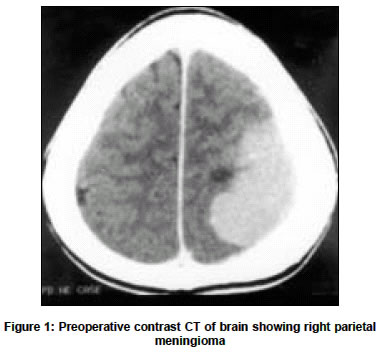
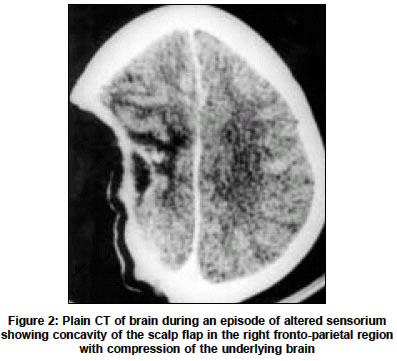
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 504-505 Short Reports Unusual presentation of the “syndrome of the trephined” Sujit Kumar GSamson, Chacko AriG, Rajshekhar Vedantam Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632004 Code Number: ni04169 ABSTRACT A 45-year-old lady underwent right fronto-parietal craniotomy and subtotal excision of a parasagittal meningioma. Bone flap was not replaced as it was infiltrated by the tumor. In the postoperative period she developed episodes of altered sensorium associated with worsening of left hemiparesis and a sunken scalp at the site of bone defect. Computed tomography (CT) of brain showed sunken scalp flap in the right fronto-parietal region with compression of the underlying brain. A diagnosis of syndrome of the trephined was considered and her symptoms improved with cranioplasty. Pathophysiology of the syndrome of the trephined is discussed.Key Words: Craniectomy, cranioplasty, intracranial pressure. INTRODUCTION Patients with large skull defects look unsightly apart from being susceptible to brain injury. Moreover, skull defect can result in various symptoms of the" syndrome of the trephined "like headache, dizziness, undue fatigability, vague discomfort at the site of defect, feeling of apprehension and insecurity, mental depression and intolerance to vibration as described by Grant and Norcross.[1] We report a patient who had episodes of altered sensorium due to a skull defect that was successfully managed by cranioplasty. CASE REPORT A 45-year-old woman presented with clinical features of a right parietal mass. CT of the brain showed a right parietal dural-based mass suggestive of a meningioma [Figure - 1]. She underwent a right fronto parietal craniotomy and subtotal excision of the mass, part of the tumor in the superior sagittal sinus being left behind. The bone flap was not replaced as it was infiltrated with the tumor and an immediate cranioplasty was not done since the brain was tense. In the postoperative period she was drowsy and she developed weakness in the left upper and lower limbs. A plain CT of the brain showed increased edema in the right parietal region with midline shift to the left. Despite decongestant drugs, the patient continued to deteriorate in sensorium (GCS of 10/15- E3, M5, V2). A repeat plain CT of brain revealed an increase in the brain swelling and there were no infarcts. She was intubated and ventilated for the next 48 hours, following which there was a gradual improvement in her sensorium and left hemiparesis. She gradually improved in sensorium to a GCS of 14/15 (E4, M6, V4) and to Grade 4 muscle power in the left upper and lower limbs. Subsequently, while she was in the ward she developed episodes of altered sensorium during which she would open her eyes to pain, localize pain with her right upper limb and make incomprehensible sounds (GCS E2, V2, M5 9/15). On these occasions it was observed that there was worsening of weakness in the left upper and lower limbs, incontinence of urine and a sunken skin flap in the region of the craniectomy. These episodes occurred more frequently when she was made to sit up with gradual improvement on making her lie down. An electroencephalography during one such episode was normal and her serum sodium valproate levels were within the therapeutic range. A CT of the brain during one such episode (37th postoperative day) showed a concavity of the scalp flap with compression of the underlying brain [Figure - 2]. A diagnosis of the syndrome of the trephined was considered. She underwent a right frontoparietal cranioplasty and postoperatively there were no further episodes of altered sensroium and her left hemiparesis had improved. DISCUSSION In 1977 Yamura and Makino coined the term "syndrome of the sunken skin flap" to describe the neurological symptoms due to a craniectomy defect.[2] Progressive contralateral hemiparesis, local pain and postural headache with cognitive and functional decline due to a skull defect have been reported and early cranioplasty has been recommended to prevent these phenomena.[3],[4] Various factors like stretching of the dura and underlying cortex due to the atmospheric pressure, cicatrical changes occurring between the cortex, dura and the skin exerting pressure on the skull contents, and impairment of the venous return due to the atmospheric pressure acting on the region of skull defect with a resultant increase in the local external pressure have been implicated in the pathophysiology of the "syndrome of the trephined".[5],[6],[7] The therapeutic value of cranioplasty has been proved by various experiments. Increase in cerebrospinal fluid (CSF) and superior sagittal sinus pressure, cerebral expansion, increase in CSF motion after cranioplasty due to an increase in cerebral arterial pulsations and improvement in cerebral blood flow, cerebral metabolism and cerebral vascular reserve capacity have been demonstrated after cranioplasty.[7],[8],[9],[10] REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04169f2.jpg] [ni04169f1.jpg] |
| |||||||||

{kind=link}
{kind=link}