 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
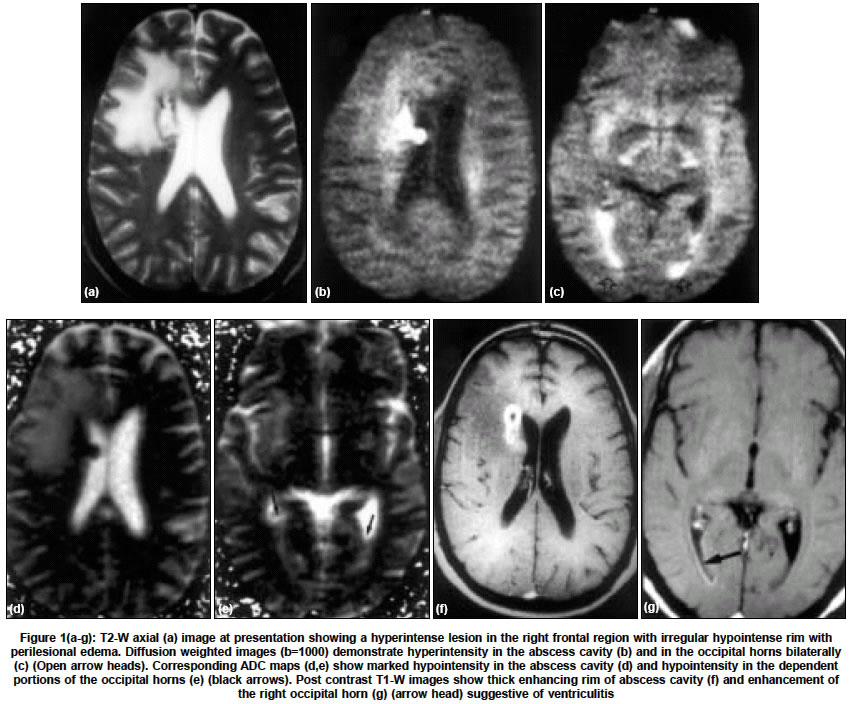
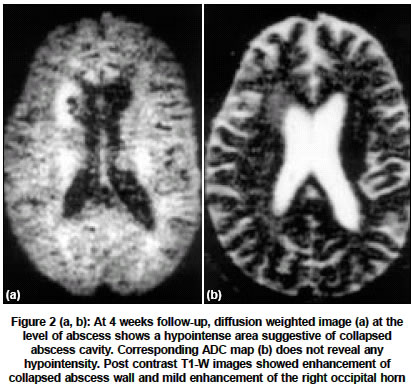
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 505-507 Short Reports Diffusion MR imaging for cerebral abscess Jati A, Venkatesh SK, Patel K, Malik S Department of Diagnostic Imaging, National University Hospital, 119074 Code Number: ni04170 ABSTRACT We report a case of cerebral abscess, which ruptured into the lateral ventricle. The radiological features on conventional MRI, appearance on both diffusion weighted images (DWI) and apparent diffusion coefficient (ADC) maps are described.Key Words: Cerebral abscess, intraventricular communication, diffusion imaging. INTRODUCTION Diffusion MR imaging can be useful in the demonstration of intraventricular rupture of a cerebral abscess.[1],[2],[3] We report the appearances of a brain abscess with intraventricular communication on diffusion weighted imaging and ADC maps at presentation and follow-up. CASE REPORT A 46-year-old male presented with low-grade fever and headache of 15 days duration. A day before presentation at our institute, there was worsening of headache associated with vomiting and impairment of consciousness. On examination he was febrile and was drowsy and irritable. There were no signs of meningitis or raised intracranial tension. There was no obvious focus of infection. Laboratory data revealed leucocytosis 18,500 cells/mm3 with 83% neutrophils. He was HIV negative. Blood cultures were sterile. MR imaging performed on a 1 Tesla machine (Harmony, Siemens, Erlangen, Germany) demonstrated a T2 hyperintense [Figure - 1a] and T1 hypointense lesion with T2 hypointense and T1 isointense rim and perilesional edema in the right frontal lobe adjoining the frontal horn of the right lateral ventricle. The lesion measured 3.3 x 1.2 x 1.0 cm in dimension. The rim was of varying thickness and appeared defective in the medial aspect with indentation on the ventricular wall [Figure - 1a]. DWI was performed with single shot axial echoplanar sequence (TR/TE, 5300/135, 5 mm thick slice, 0.3 interslice gap, 80 x 128 matrix, 230 mm field of view, 2 acquisitions; scan time 90s). Diffusion weighting was done with dual bipolar scheme. Gradient duration, 13 to 29.8 msec, distance between leading edges, 16.2 to 32.5 msec, maximum amplitude 16.4 mT/m (b=1000s/mm2). The ADC maps were generated and values calculated by using available software. DWI showed very high signal intensity in the abscess cavity which was seen to protrude into the right lateral ventricle [Figure - 1b] and there was high signal intensity in the dependent portions of the bilateral occipital horns [Figure - 1c] suggestive of abscess contents. On ADC maps [Figure - 1d,e] the abscess cavity and the dependent portions of the bilateral occipital horns appeared hypointense. The ADC value of the abscess cavity was 0.41-0.57 x 10-3 mm/sec. ADC values of the right occipital horn and the left occipital horn were 0.51-0.68 x 10-3 mm /sec and 0.65-0.76 x 10-3 mm /sec respectively. The ADC value of general cerebrospinal fluid (CSF) was 2-2.26 x 10-3 mm /sec. Post contrast T1 weighted images [Figure - 1 f,g] showed uniform enhancement of the rim except for the focal area medially. There was also enhancement of the right occipital horn [Figure - 1g] suggestive of ventriculitis. The patient was treated with broad-spectrum anti-microbial coverage. The patient showed improvement in the level of consciousness on the 3rd day of treatment and subsequently had a dramatic recovery. After 4 weeks, a repeat MRI demonstrated reduced size of the cavity. DWI revealed no hyperintensity of abscess cavity [Figure - 2]a or ventricles. The ADC maps [Figure - 2]b were normal. Post contrast T1-weighted images showed enhancement of collapsing abscess and mild enhancement of the right ventricular wall indicating persistent ventriculitis. After 8 weeks, the abscess cavity had significantly reduced in size with no abnormal signal intensity in the ventricles. ADC values of the ventricles were similar to that of the general CSF spaces. Post contrast scans showed mild enhancement in the region of the abscess cavity only. At 2 years the patient has no neurological signs or symptoms and is on follow-up. DISCUSSION Intraventricular rupture is often a fatal complication of an intracerebral pyogenic abscess and is associated with a high mortality rate of 85%.[1] The management of brain abscesses is controversial, although the uniform opinion is that early diagnosis and prompt surgical intervention is associated with a better outcome.[1] The present case was successfully managed with conservative medical treatment with regular imaging follow-up. DWI of brain has recently been studied with great interest in the characterization of brain abscess and its differentiation from other similar appearing lesions on conventional MR imaging.[4],[5] The abscesses are easily distinguished on diffusion weighted images from a cystic tumor by their high signal intensity and decreased ADC as compared to low signal intensity areas with high ADC in cases of cystic tumors.[4],[5] DWI has also been used in serial follow-up of a pyogenic abscess which demonstrated changing ADC values during treatment, but the duration of follow-up was only for 3 weeks.[6] In the present case, the patient was followed up for 8 weeks and was on conservative management. At 8 weeks, there was no hyperintesity in the abscess cavity and ventricles suggesting resolution of the purulent contents. In conclusion, DWI and ADC maps best demonstrate intraventricular rupture of an abscess. The presence of pus elsewhere can also be detected by DWI. Serial DWI with ADC maps during the management of cerebral abscess helps in assessing the response to treatment. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04170f2.jpg] [ni04170f1.jpg] |
| |||||||||

{kind=link}
{kind=link}