 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
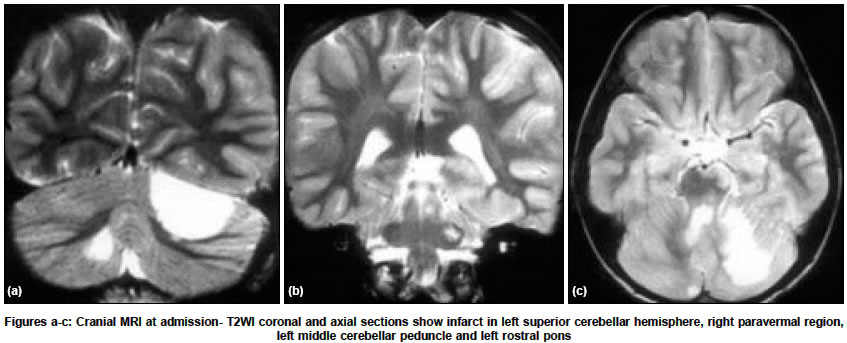
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 510-511 Letter To Editor Transient mutism due to posterior circulation infarction Nandagopal R, Krishnamoorthy SG Department of Neurology, Sri Venkateswara Institute of Medical Sciences, Tirupati, Andhra Pradesh Code Number: ni04172 Sir, Verbal mutism is described as the speechless state in a cognitively alert patient, without buccolingual apraxia. It has been a well-documented complication of resective surgery for posterior fossa tumors, especially in children.[1],[2] However, there are only few reports of posterior fossa mutism that are not due to neuro-trauma or neuro-surgical trauma.[3],[4],[5] We report the case of transient mutism in the setting of non-traumatic posterior circulation infarction. An 11-year-old boy, who was right handed, developed recurrent bouts of vomiting, giddiness, right hemiparesis, left upper limb incoordination and loss of speech, one day prior to presentation. There was no preceding history of fever, headache, neck pain or trauma. On admission, his blood pressure was normal. He was drowsy; moving left upper and lower limbs spontaneously, but could not vocalize any phoneme. He had evidence of unilateral pyramidal sign in the form of right extensor plantar response. The following day, he was more alert. He had left hemiataxia on testing for limb co-ordination with repeated coaxing, but no nystagmus. Though mute and withdrawn, he exhibited inconsolable whining for several hours. Swallowing, chewing, facial, tongue and neck movements were normal. Diagnostic investigation revealed normal findings on serum biochemistry, hemogram, erythrocyte sedimentation rate, sickling cell test, lipid profile and anti-phospholipid antibody work-up. Electro-cardiogram, echocardiography, carotid and vertebral doppler scan and X ray cervical spine were normal. Plain and contrast enhanced brain computed tomography imaging (CT scan) obtained on the day of admission, revealed multiple hypodensities involving part of left cerebellar hemisphere, right paravermal region, and left rostral pons. Brain magnetic resonance imaging (MRI) performed subsequently revealed hyperintense areas involving left superior cerebellar hemisphere, right paravermal region, left middle cerebellar peduncle and baso-tegmental region of left rostral pons on T2WI and FLAIR sequences [Figure - 1a,b,c]. Magnetic resonance angiogram (arterial and venous study) of the intracranial vasculature was normal. He was treated with aspirin and was placed on regular rehabilitation programme. There was gradual improvement of right hemiparesis in the first week. He could verbalize monosyllables in the third week and ill-articulated single words in the fourth week of illness. The subsequent slurred speech was slow and the words were uttered laboriously with strained voice and audible respiration. Gait was ataxic and broad based requiring one-person assistance. When examined two months later, his speech was near normal, the behavioral alteration had subsided and he could walk without assistance. Repeat cranial MRI scan revealed marked regression in the size of the right paravermal lesion (probably resolution of edema) and persistence of other infarcts, which became well delineated. Our patient presented with transient mutism, behavioral alteration and cerebellar and right pyramidal tract signs in the setting of multiple infarcts involving the cerebellum, left middle cerebellar peduncle and left rostral pons. The evolution of speech disorder from mutism to dysarthria and the characteristic behavioral disturbance with inconsolable whining, in the absence of dysphagia or oral apraxia, anytime during the course of illness, indicated that his speech disturbance was due to transient posterior fossa mutism, also known as, cerebellar mutism. The onset and clinical course of our patient′s illness and the topography of cerebellar and brainstem lesions (infarcts), in the absence of supratentorial involvement or antecedent illness indicated posterior circulation stroke as the aetiology. The distribution of these ischemic lesions was multifocal, in the areas supplied by left superior cerebellar, left anterior inferior cerebellar and the penetrating left pontine branches of basilar arteries, thus involving the middle and distal posterior circulation territories (apart from the non-territorial right paravermal infarct). Miyakita et al.[6] reported the first case of transient cerebellar mutism after brainstem infarction following traumatic injury of right vertebral artery. However, our patient had involvement of both brainstem and cerebellar structures in the non-traumatic context. It is noteworthy that there was transient disturbance in the level of consciousness at the onset along with transient right hemiplegia and gait ataxia in both cases. This finding was in agreement with the reported association of cerebellar mutism with a spectrum of neurological deficits including pyramidal, cerebellar and eye movement signs.[1] We believe that a complex interaction of cerebellar and brainstem involvement might be the cause of mutism in our patient. One of the suggested mechanisms for postoperative cerebellar mutism includes brainstem ischemia and subsequent edema, to account for the transient nature of the syndrome.[1] The vascular basis of this syndrome in the nonsurgical setting is better exemplified by our report. The good outcome of the speech disorder (including the improvement of dysarthria with the return of near normal speech during the subsequent period of observation), despite the presence of established infarcts, could be attributed to unilateral brainstem infarction, resolution of edema or neuronal plasticity. The behavioral disturbance also normalized with the resolution of mutism. Hence recognizing this syndrome is important in informing the parents about the prognosis and rehabilitation of speech and behavioral disorder, as most of these cases were encountered in the pediatric age group. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04172f1.jpg] |
| |||||||||

{kind=link}