 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
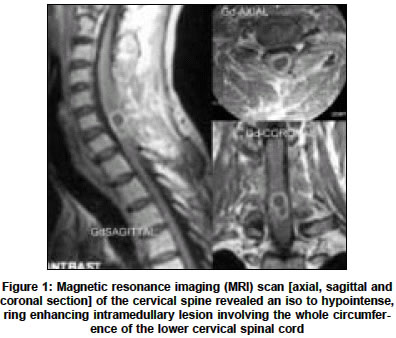
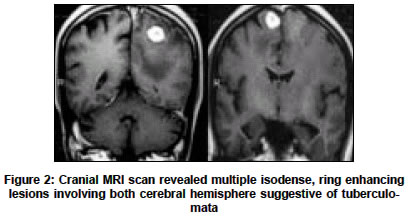
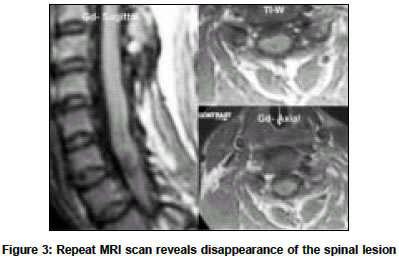
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 514-516 Letter To Editor Concurrent intramedullary and intracerebral tuberculomas Shenoy SN, Raja A Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal - 576 119, Udupi, Karnataka Code Number: ni04177 Sir, Eventhough central nervous system tuberculosis is an uncommon entity affecting 0.5% to 2% of patients with systemic tuberculosis, intracranial tuberculomas account for significant number of intracranial mass lesions in developing countries.[1] However, intramedullary tuberculomas are very rare, seen at a rate of 2/1000 cases of central nervous system tuberculosis. The incidence of concurrent spinal and cerebral tuberculomas is still very rare with less than ten cases reported in the literature.[2],[3],[4],[5],[6] An interesting case of concurrent spinal and cerebral tuberculoma who manifested simultaneously as acute quadriplegia and seizures reported here. A 38 years old gentleman presented with sudden onset of weakness of all the four limbs of two weeks duration associated with retention of urine. Neurologically, his motor system examination revealed flaccid quadriplegia with grade 3/5 power proximally in both upper limbs and grade 0/5 power in both lower limbs with brisk deep tendon reflexes and extensor plantar response. Sensory examination revealed graded sensory loss below C5 dermatome. His hematological examination revealed Hb= 12 gms/dl., WBC count = 6700/cu.mm and ESR= 40 mm/hour. Montoux and HIV tests were negative. His chest x-ray revealed no abnormality. Magnetic resonance imaging (MRI) scan of the cervical spine revealed an iso to hypointense, ring enhancing intramedullary lesion involving the whole circumference of the lower cervical spinal cord [Figure - 1]. During the hospital stay, he developed an attack of primary generalized tonic clonic seizures. His cranial MRI scan revealed multiple isodense, ring enhancing lesions involving both cerebral hemisphere suggestive of tuberculomata [Figure - 2]. He underwent C4 to T1 laminectomy. The lesion was causing the segmental enlargement of the cord and replacing the cord circumferentially. It was firm in consistency peripherally and avascular, yellowish and cheesy in the center. The lesion was excised subtotally as it was totally replacing the whole cord tissue. Postoperatively, he was continued on steroid and antituberculous therapy continued. Histopathological examination of the lesion confirmed typical tubercular granuloma. At 18 months follow-up, patient did not showed any neurological improvement and having spastic quadriplegia despite the disappearance of spinal lesion radiologically [Figure - 3]. Tuberculomas develop following haematogenous dissemination of bacilli from an infection elsewhere in the body, usually lung. Intracranial tuberculomas continue to be a serious complication of central nervous system tuberculosis affecting.[1] The spinal cord is much less commonly involved than the brain at a ratio of approximately 1:42.[7] However, concurrent spinal and cerebral tuberculomata is extremely rare and only few case reports were found in the literature.[2],[3],[5] Multiple central nervous system tuberculoma is commonly associated with human immunodeficiency virus (HIV) infection.[1] However the case reported here neither had HIV infection nor evidence of systemic tuberculosis. Intracranial tuberculomas can sometimes develop or increase in size despite administration of appropriate therapy.[8] Similarly, cases of multiple intramedullary spinal tuberculomas developing paradoxically during effective treatment of tuberculous meningitis are also described in the literature.[8] Paradoxical enlargement or development of tuberculomas usually does not represent failure of antituberculous therapy. The diagnosis of tuberculoma is usually made based on pathology, neuroimaging or clinical response to tuberculous chemotherapy. The intramedullary spinal tuberculoma although a rare entity, must be considered in the differential diagnosis of the spinal cord compression in patients with a history of systemic tuberculosis and/or human immunodeficiency virus infection.[3],[4],[7] The MRI features of the tuberculomas are distinct from other intramedullary lesions and are reliable enough to start antituberculous therapy.[2],[3],[6] Similarly MRI scan is also useful to monitor the response to treatment especially when conservative treatment is advised.[6] Most of these lesions usually resolve completely with antituberculous therapy[6] and surgical excision of the lesion is advised in patients with mass effect and paradoxical enlargement of the tuberculoma.[7],[8] However our patient did not improve despite surgical excision followed by antituberculous treatment. The failure to respond to the treatment in our case is probably multifactorial, namely, delay in instituting treatment, vascular involvement over and above an extensive intramedullary tuberculomas replacing whole circumference of the spinal cord. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04177f2.jpg] [ni04177f1.jpg] [ni04177f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}