 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
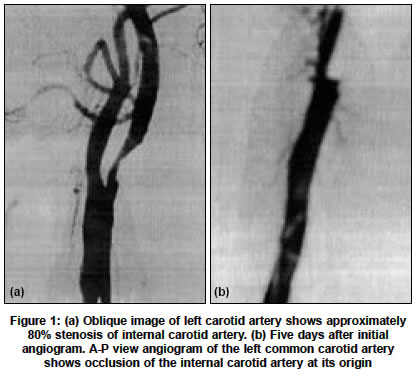
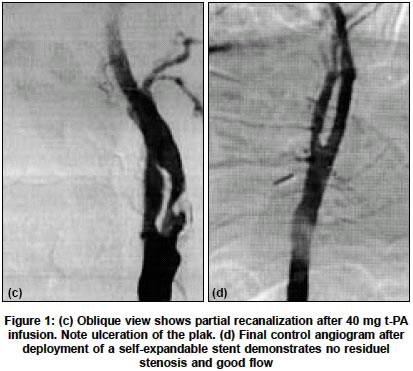
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 516-517 Letter To Editor Acute occlusion of internal carotid artery: Thrombolysis and stent placement Ciftci Ercument, Efendi Husnu, Kanko Muhip, Kutluay Pervin Departments of Radiology, University of Kocaeli, School of Medicine, 41100, Derince, Kocaeli Code Number: ni04178 Sir, Endovascular treatment of the carotid artery occlusion with balloon angioplasty-stenting and intra-arterial thrombolysis is being increasingly accepted as a treatment for acute stroke. A 61-year-old right-handed man presented with history suggestive of transient ischemic attacks 10 days ago. A clinical examination revealed no neurological deficits. An MR imaging revealed a small old lacunar infarction. Carotid angiography revealed 80% left carotid artery stenosis and 20% right carotid artery stenosis with normal intracranial circulation [Figure - 1a]. Two days after the procedure, the patient developed an acute onset of aphasia and right hemiplegia. Neurological examination showed a NIH stroke score of 19. Emergent angiography showed occlusion at the ICA origin [Figure - 1b]. No external-to-internal collaterals and leptomeningeal collaterals were present and no filling of the middle cerebral artery territory and lenticulostriate artery was observed. An exchange guidewire was passed through the diagnostic catheter and introducer was changed with 9F sheath introducer system. After a bolus of 5000 IU of heparin, a continuous heparin infusion was started. A 9F guiding catheter was placed into the common carotid artery over a 0.035-in, 300-cm guidewire positioned in the ipsilateral external carotid artery. A Tracker-18 microcatheter (Target therapeutic, Los angeles, CA, USA) was advanced over a Transend EX 0.014-in microguidewire (Boston Scientific). Microcatheter was embedded into the thrombus and a bolus of 20 mg t-PA (Alteplase) was given in 5 minutes. A partial recanalization was obtained. Before starting stenting a control angiogram showed re-occlusion. Another 20 mg t-PA was administered and recanalization was obtained [Figure - 1c]. The stenosis was crossed with 0.014-in exchange guidewire. Predilation of the carotid artery stenosis was not performed. Protective device was not used. A self-expandable 7 x 40 mm SMART (Cordis) stent was deployed across the carotid stenosis. Postdilation was performed with a 5-mm balloon. Final control angiogram revealed a patent ICA and good intracranial circulation [Figure - 1d]. Twenty-four hours later a carotid Doppler ultrasound demonstrated patent left carotid artery with normal spectral flow. Three-month follow-up showed that the ICA remained patent. Carotid occlusive disease is responsible for approximately 25% of stroke cases. Angioplasty and stenting are minimally invasive techniques and are gaining wider acceptance. Angioplasty has been tempered by the increased risk of stroke resulting from distal embolization, vessel dissection, or arterial rupture. Stenting has been shown to increase the safety and efficacy of balloon angioplasty. Stent technology has evolved and new stents that have more flexibility and radial force were introduced.[1],[2] Thrombolytic therapy for the occlusion of the ICA should be started within 6 hours after the onset of stroke.[3] Intra-arterial thrombolysis offers early recanalization with relatively low dose of t-PA. The direct application of thrombolytic drug allows a lower total dose, may reduce systemic effects and may reduce time to recanalization.[4] Intracranial thrombolysis has been performed using direct thrombolysis. Intra-arterial delivery of highly concentrated drug and mechanical disruption of the thrombus by the catheter and guidewire may have advantages over the intravenous administration.[1] Reopening of the occluded carotid arteries is controversial, and neither surgical nor endovascular treatment of complete ICA occlusion has become standard practice. For patients with chronic occlusions, successful reopening of the ICA is highly unlikely. However, in acute occlusion, emergency surgery to perform a thromboendarterectomy using Fogarty catheter to pull thrombus can yield good results.[5] Bellon et al have used a device to open occluded ICA to reach MCA occlusion to obtain flow.[6] PTA and stenting of the carotid arteries are associated with an obligatory release of particulate debris into the distal cerebral circulation. Although most of the emboli are small and do not cause symptomatic neurological deficit, some may be large enough to result in stroke. For this reason cerebral protection with occlusive balloon, filter, flow-reversal is used to decrease the risk of distal embolizastion during PTA and stenting.[2],[7],[8] REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04178f1a-b.jpg] [ni04178f1c-d.jpg] |
| |||||||||

{kind=link}
{kind=link}