 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
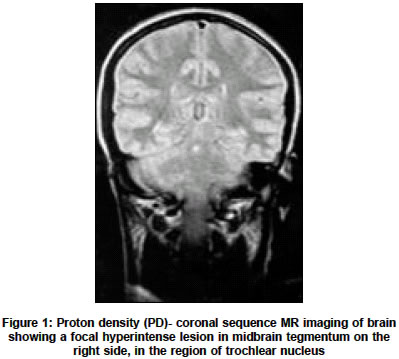
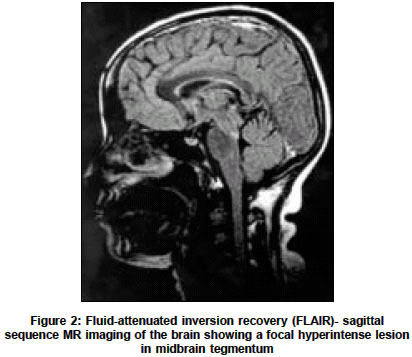
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 517-518 Letter To Editor Isolated internuclear ophthalmoplegia as a manifestation of an isolated inflammatory demyelinating lesion of the brainstem Kumar Sudhir, Aaron S Neurology Unit, Department of Neurological Sciences, Christian Medical College, Vellore - 632004, Tamil Nadu Code Number: ni04179 Sir, Internuclear ophthalmoplegia (INO), an uncommon clinical sign, is more frequently described in association with multiple sclerosis (MS).[1],[2] However in patients with MS mild to moderate INO can be missed on clinical examination.[3] Detection of a lesion in medial longitudinal fasciculus (MLF) depends upon the appropriate choice of magnetic resonance imaging (MRI) sequences.[4] We present a patient with isolated unilateral INO probably due to an isolated inflammatory demyelinating lesion of the brainstem. A 34 year-old otherwise healthy lady presented with two-day history of diplopia on left gaze. Otherwise the history was unremarkable. There was no fever or vaccination before the onset of the symptoms. Clinical examination showed right-sided INO with normal convergence. She did not have any other neurologic deficit. MR imaging of the brain revealed a focal hyperintense lesion in the right midbrain tegmentum (in the region of trochlear nucleus) [Figure - 1], [Figure - 2]. Cerebrospinal fluid analysis (CSF) showed normal biochemistry and a cell count of 5 lymphocytes. CSF was negative for oligoclonal bands. Routine blood biochemistry and hemogram including erythrocyte sedimentation rate at first hour, collagen profile were normal. Tests for retroviral serology were negative. Electrodiagnostic tests, nerve conduction studies, visual, somatosensory, and brainstem auditory evoked potentials were normal. Based on the MRI finding, she was diagnosed as a case of inflammatory demyelinating disorder and was treated with intravenous methylprednisolone, 1 g/day per 3 days. She had a partial improvement. Internuclear ophthalmoplegia is a distinct clinical sign and seen in association with a lesion in the MLF between the third and sixth cranial nerve nuclei (midbrain or pontine tegmentum). The causes of INO include MS, brainstem stroke, brainstem tumor, metastases, traumatic brain injury, central nervous system infections including neurosyphilis, Arnold-Chiari malformation with associated syringobulbia, Wernicke′s encephalopathy, and hepatic encephalopathy.[5] In our patient all the other possibilities other than demyelinating pathology were excluded. She did not have any prodromal illness or vaccination before the onset of the illness and no other white matter MRI lesions. We feel that our patient is probably a case of primary demyelinating disease, possible MS. The newly revised MRI diagnostic criteria for MS allow the diagnosis to be made after one attack, if stringent MRI criteria are met. It has been emphasized that in patients with first attack of demyelinating disease, a diagnosis should be withheld unless new symptoms and signs or imaging abnormalities appear, more than 3 months after the onset of clinical symptoms.[6] Clinical examination fails to detect INO in 71% and 25% of the cases with mild and moderate INO respectively, and detection is improved by quantitative infrared oculography.[3] MRI is the imaging modality of choice to detect the lesions of MLF.[7] In MS patients with INO, hyperintense lesions in MLF have been demonstrated in all patients on PD sequence, in 88% on T2-weighted imaging and in 44% on FLAIR sequences.[4] In our patients the lesion in the MLF was detected only on PD coronal and FLAIR. Thus our recommendation in patients is to acquire PD sequence in addition to the other sequences in a patient with suspected INO. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04179f2.jpg] [ni04179f1.jpg] |
| |||||||||

{kind=link}
{kind=link}