 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
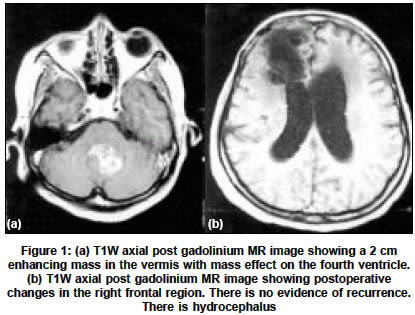
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 521-522 Letter To Editor Metastasis of frontal oligoastrocytoma to cerebellar vermis Sujit Kumar GSamson, Chacko Geeta, Rajshekhar Vedantam Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632 004, Tamilnadu Code Number: ni04184 Sir, Metastasis of a low-grade glioma through the cerebrospinal fluid (CSF) is very rare. We report a case of CSF spread of a right frontal oligoastrocytoma to cerebellar vermis. A 46-year-old woman presented with symptoms of raised intracranial pressure and difficulty in walking of two months duration. On examination, she had bilateral papilloedema and cerebellar signs on the left side. Four years earlier she had undergone excision of right frontal mixed oligoastrocytoma (WHO Grade 2) followed by 54 Gy of Cobalt teletherapy to the brain. Magnetic resonance imaging (MRI) of the brain showed a 2 cm homogeneous contrast enhancing mass in the inferior vermis with extension into the left cerebellar hemisphere and hydrocephalus. There were postoperative changes in the right frontal lobe in the form of loss of brain tissue and there was no evidence of recurrence [Figure - 1a and b] . A differential diagnosis of metastases from a systemic tumor, CSF spread of the frontal glioma or radiotherapy-induced tumor were considered. On referring to her previous radiotherapy records it was found that the posterior fossa was not included in the radiation field. Chest X-ray and an ultrasound abdomen were normal. She underwent right ventriculoperitoneal shunt followed by midline suboccipital craniectomy and radical excision of the mass. The biopsy was reported as oligoastrocytoma (WHO Grade 2). She was given 56 Gy of external radiotherapy. Choucair et al, in a large study, have reported the frequency of CSF metastases at 5-7%.[1] Compared to malignant primary tumors of the central nervous system low-grade gliomas are rarely known to metastasize through the CSF. In 1929, Cairns[2] reported the first case of CSF spread of an oligodendroglioma through the ventricles. In our case, similar histology of the frontal and vermian masses, rarity of primary vermian mixed oligoastrocytoma and the fact that the vermis was not included in the radiation field after the first surgery suggest that the vermian mass is likely to be due to CSF spread. The possible mechanisms of tumor dissemination include exfoliation of cells into the CSF of the ventricles or the subarachnoid spaces. Previous craniotomy procedures, shunt procedures, site of tumor, glioma type and tumor cell differentiation are known to affect CSF spread of gliomas.[3],[4],[5] Oligodendrogliomas are more commonly associated with CSF dissemination. Friedberg et al[6] have proposed CSF analysis of specific matrix metalloproteinases profile as a means to detect CSF spread of tumors. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04184f1.jpg] |
| |||||||||

{kind=link}