 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
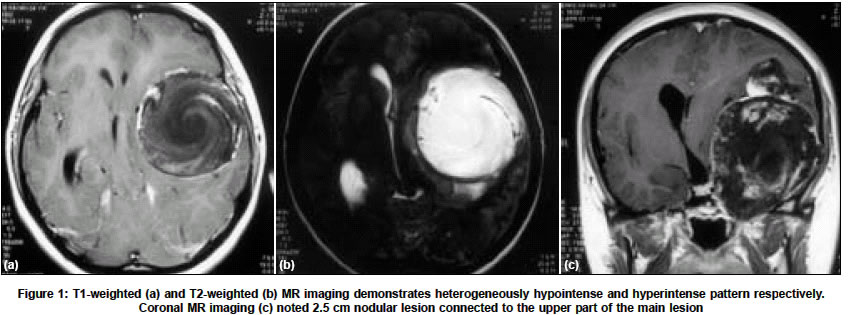
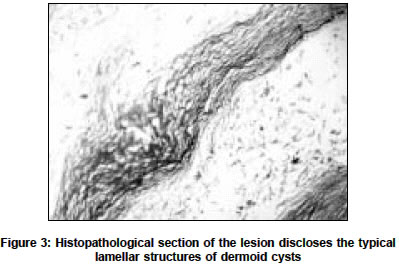
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 524-525 Letter To Editor Intracranial dermoid cyst mimicking a giant thrombosed aneurysm Canbaz Bulent, Kemerdere Rahsan, Ocal Eylem, Tanriverdi Taner Department of Neurosurgery, Istanbul University, Cerrahpasa Medical Faculty, Istanbul, P. K. 4, 34301, Cerrahpasa-Istanbul Code Number: ni04187 Sir, Dermoid tumors are dysembryogenetic cysts derived from ectodermal inclusions of primitive pluripotent cells.[1] They frequently occur in the midline, but parasellar and frontobasal regions are also involved.[2],[3] We describe a case with histopathologically proven intracranial dermoid cyst which resembled a giant thrombosed aneurysm. A 24-year-old female had severe headache and left earache for 4 months. There was no other symptom. Neurological examination revealed no evidence of focal deficit, but the patient had hyperactive right deep tendon reflexes, and positive Hoffmann and Babinski sign on the right side. Plain CT scan showed an approximately 7.5 x 7 x 6.5 cm iso-hypodense mass located in the left temporal lobe. MRI, showed an extra-axial lesion, which was heterogeneously hypointense on T1-weighted and hyperintense on T2-weighted images [Figure - 1a, b]. The images suggested lamellar organized hemorrhagic components within the lesion. Another 2.5 cm nodular lesion was connected with a narrow neck to the superior part of the main lesion [Figure - 1c]. There was no lesion surrounding edema. DSA was done as the imaging features mimicked a giant thrombosed aneurysm. It did not reveal any vascular abnormality [Figure - 2]. At surgery, a dermoid tumor with hair follicles and keratin like material was identified and was radically resected. The patient was well after surgery and postoperative CT scan showed no residual tumor. Histopathological examination confirmed that the lesion was a dermoid cyst [Figure - 3]. Dermoid cysts are well-circumscribed lesions lined by stratified squamous epithelium. They include a viscous greenish brown fluid, which comprises lipid metabolites, whorls of hair, calcifications, and decomposed epithelial cells.[2],[4] These contents of the cyst determine its characteristic appearance on MRI studies. They are usually hypodense on plain CT scan. The magnetic resonance appearance includes typical high signal intensity on T1-weighted images and variable signal ranging from hypo to hyperintensity on T2-weighted images.[3] The fat content is seen strongly hyperintense on T1-weighted imaging while the other contents appear hypointense. On T2-weighted sequences, the fat component demonstrates hypointensity similar to subcutaneous fat.[3],[5] A thin rim of calcification is frequently present.[5] Additionally, curvilinear hypointense elements may be seen if the lesion contains hair. The mixed composition of the tumor gives it a characteristic non-homogenous appearance.[2] A giant thrombosed aneurysm was considered preoperatively due to the unusual location and the lamellar pattern of the lesion simulating a clot in different stages of organization.[6] REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04187f3.jpg] [ni04187f2.jpg] [ni04187f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}