 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
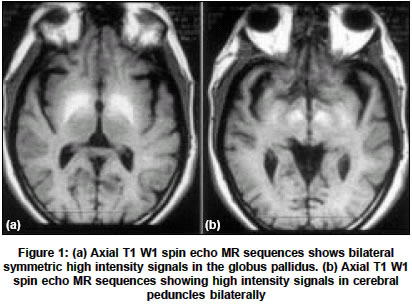
Neurology India, Vol. 52, No. 4, October-December, 2004, pp. 527 Neuroimage Acquired (Non-Wilsonian) hepatocerebral degeneration Khan FiroshS, Ashalatha R Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum Code Number: ni04189 A 65-year-old man presented with progressive symmetric, akinetic rigid syndrome with postural tremors and postural instability of one-year duration. He also had marked apathy and abulia and mild recent memory impairment. This syndrome was punctuated by fluctuations in both motor and cognitive functions with ′good′ as well as ′bad′ days lasting 24-48 hours. During one such delirious spell, he presented to us. Clinical examination revealed a hypokinetic delirious state, with symmetric bradykinesia and cogwheel rigidity. There were bilateral release reflexes, with no other lateralizing signs, general physical examination including KF ring were negative. Investigations revealed deranged liver function s with elevated serum ammonia and diffuse theta slowing on scalp EEG. MRI brain (1.5T) revealed bilateral symmetric T1 hyperintensities (T1H1) involving bilateral globus pallidi (GP), tectum of pons and midbrain, crus cerebri and substantia nigra (SNG) with sparing of red nuclei [Figure - 1]. T2WI did not reveal any abnormality. Patient was treated with hepatic coma regime and his sensorium improved to near normalcy, although no major change in his motor functions was observed. Bilateral pallidal T1HI should prompt to investigate for a hepatocellular disease since it occurs in more than 75% of patients with cirrhosis irrespective of the presence or absence of neurologic symptoms.[1],[2] In a series of 11 patients with parkinsonian features and cirrhosis, all patients had this imaging feature,[1] which is quite often under diagnosed. Other than GP, the preferred sites of involvement are SNG, ventral midbrain, quadrigeminal plate, anterior pituitary, hypothalamus, subthalamic nucleus etc.[1],[3] Putamen, caudate nucleus, thalamus, red nucleus and cerebellum are usually spared as in our case. The proposed mechanism of this TIHI in MRI are many, but the most valid one is the deposition of manganese with its paramagnetic effect which also explains the clinical manifestations secondary to basal ganglia dysfunction caused by manganese.[4] Cirrhosis-related Parkinsonism thus represents a unique, rare, acquired hepatocerebral degeneration (AHD), different from acute hepatic encephalopathy and classical Parkinson′s disease. AHD is a neurologic syndrome associated with a chronic hepatic disease with history of acute to subacute worsening with disturbance of consciousness ranging from confusion, stupor, coma and even death. Such episodes are rather rare in Wilson′s disease. The age at presentation is also earlier for Wilson′s disease, in the 2nd to 3rd decade whereas for AHD it is still later. This features along with an absence of KF ring, normal serum ceruloplasmin and copper and urinary copper favor the diagnosis of AHD. The cerebral MR appearance of Wilson′s disease can range from normalcy to bilateral symmetrical grey matter lesions in caudate, lenticular, thalamic and dentate nuclei (usually hypo in T1, hyper/hypo or both in T2). The mesencephalon involvement with the characteristic ′Giant Panda sign′ of Wilson′s has never been reported in AHD. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04189f1.jpg] |
| |||||||||

{kind=link}