 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
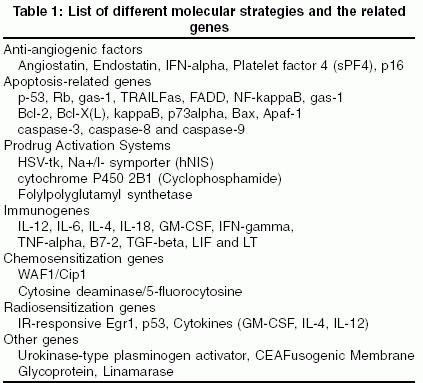
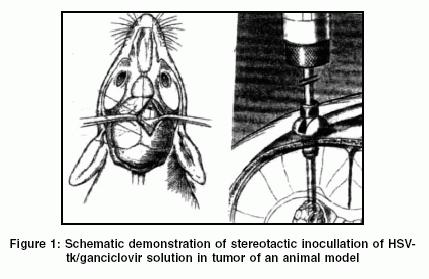
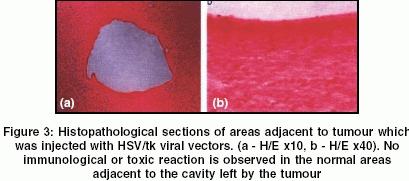
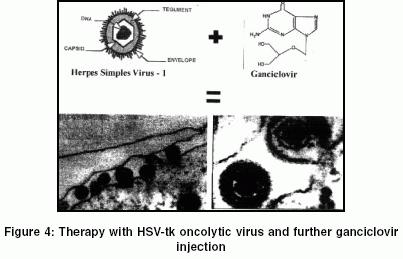
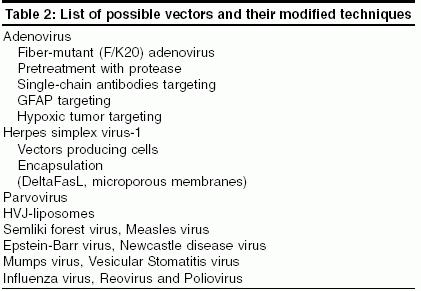
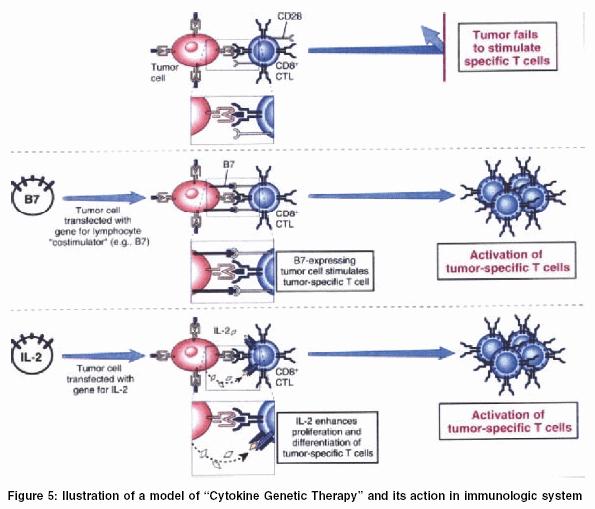
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 17-26 Review Article Genetic therapy in gliomas: Historical analysis and future perspectives Mattei TobiasAlecio, Ramina Ricardo, Miura FlavioKey, Aguiar PauloHenrique, Valiengo Leandroda Costa Department of Neurosurgery, Sao Paulo Medical School Code Number: ni05003 Abstract High-grade gliomas are relatively frequent in adults, and consist of the most malignant kind of primary brain tumor. Being resistant to standard treatment modalities such as surgery, radiation, and chemotherapy, it is fatal within 1 to 2 years of onset of symptoms. Although several gene therapy systems proved to be efficient in controlling or eradicating these tumors in animal models, the clinical studies performed so far were not equally successful. Most clinical studies showed that methodologies that increase tumor infection/transduction and, consequently confer more permanent activity against the tumor, will lead to enhanced therapeutic results. Due to the promising practical clinical benefits that can be expected for the near future, an exposition to the practicing neurosurgeon about the basic issues in genetic therapy of gliomas seems convenient. Among the main topics, we shall discuss anti-tumoral mechanisms of various genes that can be transfected, the advantages and drawbacks of the different vectors utilized, the possibilities of tumor targeting by modifications in the native tropism of virus vectors, as well as the different physical methods for vector delivery to the tumors. Along with the exposition we will also review of the history of the genetic therapy for gliomas, with special focus on the main problems found during the advancement of scientific discoveries in this area. A general analysis is also made of the present state of this promising therapeutic modality, with reference to the problems that still must be solved and the new paradigms for future research in this area. Key Words: Genetic transduction, genetic vectors, history, maligant gliomas, transfection. Introduction In adults, gliomas are devastating diseases, with very few chances of survival, despite the lack of distant metastases. The best available treatments, such as surgical resection and radiotherapy, have been only temporarily successful. This happens because with the post-resection tumor residues, which are almost always present, it becomes fatal within 1 to 2 years of the first onset of symptoms.[1]The two factors that promote the use of gene therapy for gliomas are the failure and toxicity of conventional therapies, as well as the identification of genetic abnormalities which contribute to the malignancy of gliomas. Uncontrolled cellular proliferation, lack of apoptosis, invasion, and angiogenesis are among the biological processes that make these tumors both aggressive and difficult to treat.[2] During the malignant progression of gliomas, several tumor suppressor genes are inactivated, and numerous growth factors and oncogenes are overexpressed progressively. Consequently, gliomas′ gene therapy may aim at molecular interference with ′gain of function′ genes (oncogenes) or replacement of ′loss of function′ genes (tumor suppressor genes). Such approaches require transgene expression in entire tumor cell populations (if other mechanisms do not come into play) which cannot be achieved with current vector systems. Hence, other strategies have been pursued that may be independent of the genes actually involved in tumor genesis [Table - 1]. Microbial genes (e.g. herpes simplex virus thymidine kinase) may be transferred into the tumors allowing prodrug activation (e.g. ganciclovir). Furthermore, cytokines or other immunomodulatory genes may be used for vaccination purposes, which frequently involves ex vivo transfection of autologous tumor cells with such genes. Malignant gliomas were chosen for the first clinical study on new gene therapy approaches because these tumors are non-metastatic and develop on the largely post-mitotic background of normal glial and neuronal tissue. Several molecular strategies have been tested, either in animal models or clinical trials: prodrug activating systems, introduction of tumor suppressor or cell-cycle-related genes, inhibition of growth factors and/or their receptors, inhibition of neovascularization, immunomodulatory maneuvers, oncolytic viruses, inhibition of matrix metalloproteinases, induction of toxic agents and sensitization of tumors of local expression to chemotherapeutic agents and radiotherapy.[3],[4] There are different physical methods for vector delivery to malignant primary brain tumors in experimental or clinical settings: stereotactic or direct intratumoral injection or convection-enhanced bulk-flow interstitial delivery; intrathecal and intraventricular injection; intravascular infusion with or without modification of the blood-tumor-barrier; and direct intra-tumoral delivery of anti-sense oligonucleotides.[5],[6] Critical evaluation of gene transfer and therapy studies has led to the conclusion that even using identical vectors, the anatomical route of the vector can dramatically affect both the efficiency of tumor transduction and its spatial distribution, as well as the extent of intratumoral and intracerebral transgene expression. The safety and efficiency of these therapeutic systems in humans has been confirmed by several controlled pre-clinical and clinical therapeutic trials.[7],[8],[9] Genes Prodrug Activation Systems HSV-TK/GanciclovirTumor cell transduction with the herpes simplex virus thymidine kinase (HSV-TK) gene and treatment with ganciclovir (GCV) is the most widely studied cancer gene therapy.[10],[11],[12],[13],[14] HSV-TK converts the prodrug ganciclovir (GCV) into a toxic nucleotide analogue, whose incorporation into cellular DNA blocks cell proliferation. Following repetitive ganciclovir (GCV) intraperitoneal or intravenous injection, effective killing of glioma cells in mouse brain is observed. There are several techniques described in the literature for the HSV-TK/GCV therapy with variations depending on the vector utilized, and the concentration of injection solution. We will describe here a standard technique which consists of the insertion, through genetic engineering techniques, of the herpes HSV-TK gene in a modified, usually replication-defective, viral vector (adenovirus or retrovirus). About 3 microliters of a solution with titers of approximately 1.4-2.5 x 1011 colony-forming units (cfu)/ml of the viruses containing the HSV-TK gene is stereotaxically inoculated into the tumor. [Figure - 1].[15],[16] This method results in highly efficient transduction in vivo, as documentation studies of gene expression using positron emission tomography show.[17] The inoculation is followed, 3 days later, by intraperitoneal or intravenous injection of GCV for 10 days. The in vivo studies relate a significant regression of the tumors in 50-80% of the rats treated with this technique, if compared to control animals. In some animals, the tumor completely disappeared after this treatment protocol and the mice were completely cured[17],[18],[19],[20] [Figure - 2] and [Figure - 3]. Tissue reactions after 14 days of GCV treatment are characterized by astrogliosis and apoptosis, whereas microglia response and immunoactivation of the brain cells appear to play a minor role.[21],[22] Microglia response stimulation by gene transfer or other means might improve the efficacy of the HSV-TK/GCV treatment in vivo.[23] Anti-angiogenic factors Inhibition of angiogenesis has been considered among the most promising approaches to treat highly vascularized solid tumors, such as high-grade gliomas. However, chronic systemic delivery of therapeutic proteins, such as inhibitors of angiogenesis, present several difficult pharmacological challenges. The concept that targeted anti-angiogenesis, using virally mediated gene transfer, represents a promising strategy for delivering this anti-angiogenic factors.[24]Angiostatin, Endostatin, and IFN-alpha(1) Some researchers evaluated the effects of local production of three endogenous inhibitors of angiogenesis (angiostatin, endostatin, and interferon (IFN)-alpha(1)), using a stably transfected rat (9L) and human (GL15) glioblastoma cells, on tumor vascularization and growth in an in vitro assay system based on the implantation of tumor cells into organotypic brain slice cultures. Although all the three genes showed angiogenesis inhibitory effect, IFN-alpha demonstrated the most potent anti-angiogenic effect in organotypic brain slice cultures. In vivo, after intracerebral implantation of such genetically modified high-grade glioma cells, IFN-alpha(1) caused a dramatic decrease in tumor volume, as revealed by magnetic resonance imaging and by postmortem histology. The mechanisms of this anti-tumor effect were most likely caused by the major anti-angiogenic action of the cytokine, because IFN-alpha(1) expression provoked a pronounced decrease in blood vessel density, which was accompanied by extensive necrosis in the tumors′ body mass.[25] p16 gene Recent studies have indicated that the loss of p16 is a frequent event in the progression of malignant gliomas. The loss of p16 promotes the acquisition of malignant characteristics in gliomas, which are among the most angiogenic of all human tumors. High-grade gliomas are distinguished from low-grade gliomas by intense angiogenesis in addition to their frequent loss of p16. Infection with a recombinant replication-defective adenovirus vector containing the cDNA of wild-type p16, significantly reduced the expression of vascular endothelial growth factor, which is thought to be a pivotal mediator of tumor angiogenesis, in p16-deleted glioma cells. Restoring wild-type p16 expression into p16-deleted glioma cells markedly inhibited angiogenesis induced by tumor cells in vivo. Furthermore, wild-type p16 inhibited neovascularization more potently than did wild-type p53 transfer.[26] Apoptosis-related genes p-53 genep-53 gene therapy is in clinical development in the treatment of various cancers. The p53 gene is thought to function abnormally in the majority of malignant gliomas, although it has been demonstrated to be mutated in only approximately 30%. This has led to studies in which adenoviral transduction with wild-type human p53 has been investigated in an attempt to slow tumor cell growth. Some authors demonstrated that multiple gene replacements with simultaneous exposure to adenovirus-containing p53 gene can produce additive effects in the treatment of glioma cell lines.[27] Rb gene The development of high-grade gliomas involves progressive inactivation of several tumor suppressor genes. Retinoblastoma tumor suppressor gene abnormalities are found in the majority of cancers, including, at least, 30% of malignant gliomas.[28] These findings provide direct evidence that inactivation of the retinoblastoma protein is a critical event in gliomas and suggest that the restoration of wild-type retinoblastoma activity in these tumors through vector delivery gene therapy may have great therapeutic utility. Other apoptosis-related genes Some studies suggest that adenoviral vector-mediated delivery of other apoptosis-related genes may also be potentially useful in the gene therapy approach towards the treatment of human brain gliomas. The apoptosis-related genes already studied are: Fas/Fas ligand, caspase-8, p33ING1, p73alpha, Bax, Apaf-1, caspase-9, IkappaBdN, NF-kappaB, caspase-3, gas-1, Bcl-2, and Bcl-X(L).[29],[30],[31],[32],[33] Immunogenes Cancer immunogene therapy is based on vaccination with radiated, autologous tumor cells transduced with immunostimulatory genes. It has been demonstrated that high-grade gliomas produce immunosuppressive factors, like TGF-beta, which reduce the anti-tumor response by peripheral blood effector cells. These immunosuppressive factors could be neutralized to improve anti-tumor response.[34],[35],[36],[37]Vaccination treatment using genetically modified tumor cells to express certain cytokines consist in the following steps: First, glioma cells are cultured primarily from the patients′ surgically resected tumor tissues. Afterwards, in vitro infection with a recombinant virus vector containing the gene of the cytokine is procede, and afterwards, the transduced cells are re-injected in the patient.[38],[39],[40] Vaccination therapy induces specific activation of cytotoxic T lymphocytes measured by cell-mediated cytotoxicity assay, suggesting the generation of a specific anti-tumor response and the potential for systemic immunity [Figure - 4].[41],[42] This immunization results in the regression of the implanted cells, as well as the original brain tumor. Mice cured of their intracerebral tumors by this vaccination therapy also demonstrated protective immunity upon rechallenge, showing that this kind of therapy may have promising results in preventing the important problem of tumor residues, almost always present in high-grade gliomas.[43] Several cytokines have been studied: IL-12, IL-6, IL-4, IL-18, IFN-gamma, TGF-beta, TNF-alpha, GM-CSF, B7-2, TNF-alpha, LIF and LT.[44],[45] Chemosensitization genes Cell cycle regulator WAF1/Cip1Studies have shown that negative cell cycle regulator WAF1/Cip1 is often overexpressed in human gliomas and that WAF1/Cip1′s overexpression makes glioma cells resistant to chemotherapy agents. It has been investigated whether down-regulation of WAF1/Cip1 could sensitize gliomas to chemotherapy. An adenoviral vector expressing antisense WAF1/Cip1 was constructed and used to infect D54 glioma cells which express a high level of endogenous WAF1/Cip1. Down-regulation of WAF1/Cip1 alone resulted in the cells rounding up and detaching from plates. The antisense WAF1/Cip1-infected cells were then treated with the chemotherapeutic agents 1,3-bis (2-chloroethyl)-1-nitrosourea and cisplatin. Trypan blue exclusion assay revealed significant cell death in antisense WAF1/Cip1-infected cells. These results show that the attenuation of WAF1/Cip1 expression initiated glioma cell death and sensitized glioma cells to apoptosis induced by 1,3-bis(2-chloroethyl)-1-nitrosourea and cisplatin. Thus, blocking WAF1/Cip1 production may serve as a useful chemosensitization regimen for treating glioma.[46] Cytosine deaminase/5-fluorocytosine 5-Fluorouracil (5-FU) is a potent antimetabolite used in the chemotherapy for gastrointestinal (GI), breast, head, and neck malignancies. Despite initial excitement, the therapeutic index of 5-FU has been shown to be very poor. It is unclear whether this lack of utility is due to problems with drug delivery or inherent insensitivity. Adenovirus (Ad) vector-mediated cytosine deaminase (CD)/5-fluorocytosine (5-FC) gene therapy has been proposed as a potential technique to overcome pharmacokinetic issues associated with systemic 5-FU and is particularly well suited to use with tumors in which local control is paramount, such as malignant gliomas. The bacterial enzyme cytosine deaminase (CD) catalyzes the conversion of 5-fluorocytosine (5-FC) to the lethal 5-fluorouracil (5-FU). Cloning the CD gene from Escherichia coli and expression in human tumor cell lines enabled these cells to convert 3H-labeled 5-FC into 3H-5-FU. Glioblastoma cell line T1115 became 200-fold more sensitive to 5-FC than the non-expressing parental cell lines. At least 90% of the cells are killed within 7 days. CD-expressing cells are able to kill non-expressing cells when grown in the same culture flask (bystander effect). The results of clinical studies in human patients with high-grade gliomas confirm the previous findings in rat models, demonstrating the potential clinical utility of Ad 5-FC gene therapy for gliomas.[46] Radiosensitization genes Bax geneThe hypothesis that Ad-mediated transfection of proapoptotic Bax gene could enhance the cytotoxicity of radiotherapy (RT) in RT-refractory glioma cells has been proposed. The results of in vivo experiments showed that apoptotic death may be enhanced by the combination of the treatment with Ad-containing Bax gene (Ad-Bax) and RT. Remarkably, combined treatment induces regression of tumors in mice. In animals injected with subcutaneous tumors (D54 MG line), levels of apoptosis after RT alone, Ad/Bax alone, or the combination, were respectively, 12.3%, 32.1% and 78.5%. A colony-formation assay showed a 2-log inhibition with respect to controls after combined treatment, irrespective of the endogenous levels of p53.[47] These results confirms that Ad/Bax synergistically radiosensitizes glioma, with a seemingly favorable therapeutic index. Radiation-responsive gene promoters Synthetic gene promoters, responsive to clinical doses of ionizing radiation (IR), have been developed for use in suicide gene therapy vectors. A series of plasmid vectors containing different enhancer/promoters has been investigated. The crucial DNA sequences utilized are units with the consensus motif CC(A/T)(6)GG, known as CArG elements, derived from the IR-responsive Egr1 gene. These elements had their sequences incorporated into a synthetic gene promoter and assayed for the ability to induce expression of a downstream reporter gene following irradiation. Exposure of cells to ionizing radiation resulted in the activation of these specific transcriptional control elements within the early growth response 1 (Egr1) gene promoter, leading to increased gene expression. Studies revealed that increasing the number of CArG elements up to a certain level, increases promoter radiation-response; specific alteration of the core A/T sequences caused an even greater positive response.[48] These enhancers can be used to drive suicide gene expression from vectors delivered to a tumor within an irradiated field. These results demonstrate that the synthetic promoter is responsive to low doses of ionizing radiation, and therefore, isolated CArG elements function as radiation-mediated transcriptional enhancers outside their normal sequence context. The continued development and optimization of such radiation-responsive synthetic promoters is expected to make a valuable contribution to the development of future radiation-responsive vectors for cancer gene therapy. p53 gene There are studies in which adenoviral transduction with wild-type human p53 has been demonstrated to slow tumor cell growth.[49] During the investigations in p53 gene therapy, it has also been suggested that adenoviral vector-mediated expression of human wild-type p53 could not only slow tumor cell growth but also enhance the radiosensitivity of malignant glioma cells that express native wild-type p53. It was demonstrated that RT2 tumor cells express native rat wild-type p53 before the transduction, and markedly overexpressed human p53 following adenoviral p53 transduction. The combination of p53 transduction followed by radiation resulted in marked decreases of RT2 cell survival and increases in apoptosis at radiation doses from 2 to 6 Gy. Animals receiving cranial radiation after intracerebral implantation with RT2 cells previously transduced with p53 survived significantly longer than control animals.[50] These results support a new perspective in the p53 genetic therapy, showing the ability to enhance the radiosensitivity of malignant glioma cells that express wild-type p53 by using adenoviral transduction to induce overexpression of p53. This offers new hope for the p53 viral-mediated genetic therapy as a successful therapeutic strategy, not only in human gliomas that express mutant p53, but also in those that express wild-type p53. Cytokines Some cytokine vaccination (GM-CSF, IL-4, IL-12) therapies have not only primary immunity generation against the tumor but also an important radiosensitization effect. In some studies with tumors treated with vaccination therapy and posteriorly, irradiation, about 80-100% of the glioma-bearing mice were cured. Other genes Other genes which have been evaluated as candidates for genetic therapy in gliomas are: folylpolyglutamyl synthetase gene, growth arrest-specific genes (gas1), tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), cell cycle regulator WAF1/Cip1 gene, cytosine deaminase/5-fluorocytosine gene, Bax gene, carcinoembryonic antigen (CEA) gene, urokinase-type plasminogen activator gene and fusogenic membrane glycoprotein gene.[51],[52],[53],[54],[55],[56],[57]Vectors Viruses [Table - 2] have emerged on the genetic therapy scene and gained attention due to their ability to play essentially two roles: first, as vectors for therapeutic gene delivery and second, as engineered infectious agents capable of selectively lysing tumor cells.[58]Much effort in the past has been placed in using replication-defective viruses to this end, but they have shown many disadvantages. Recent attention has been focused on the potential of replication-competent viruses to discriminatingly target, replicate within, and destroy tumor cells via oncolysis, leaving adjacent post-mitotic neurons unharmed. Oncolytic viruses have shown promising results in solid tumor treatment, including gliomas, but their potency must be improved if their full clinical potential is to be realized.[59] Adenovirus The local, intratumoral injection of adenovirus is an especially suitable strategy for gliomas because these tumors, although infiltrative, rarely metastasize. Two approaches have been used to generate tumor-selective replicative adenoviruses: use of tumor-specific promoters to regulate the expression of viral genes, and the deletion of the viral functions required for the cell cycle activation.[60] Since normal cells surrounding gliomas are quiescent, the second strategy is particularly attractive to develop new treatments for brain tumors.[61] Laboratory studies showed that 20% of the rats can be cured (survival >6 months) after optimized adenovirus thymidine kinase gene therapy.[62] Trials have showed that adenoviruses are more efficient than retroviruses in achieving in vivo gene transfer.[63]Targeted adenovirus The application of adenoviral vectors in cancer gene therapy is hampered by low receptor expression on tumor cells and high receptor expression on normal epithelial cells. Targeted techniques with adenoviral vectors seem to be a promising tool for cancer gene therapy; they could provide an improved therapeutic index with efficient tumor transduction and effective protection of normal tissue.[64] Single-chain antibodies targeting Some authors proposed specific tumoral targeting by the use of doubly ablated adenoviral vectors, lacking coxsackievirus-adenovirus receptor and alpha(v) integrin binding capacities, together with bispecific single-chain antibodies targeted toward human epidermal growth factor receptor (EGFR) or the epithelial cell adhesion molecule. These vectors efficiently and selectively targeted both alternative receptors on the surface of human cancer cells. With primary glioma cell cultures, EGFR targeting augmented the median gene transfer efficiency of doubly ablated adenoviral vectors 123-fold. Moreover, EGFR-targeted doubly ablated vectors were selective for human brain tumors versus the surrounding normal brain tissue.[65] GFAP targeting In an attempt to limit the toxic effects on normal tissues, a recombinant adenoviral vector has been constructed, in which the HSV-TK gene is driven by a 2.2 kb DNA promoter which controls expression for the encoding glial fibrillary acidic protein gene (GFAP), an intermediate filament protein expressed primarily in astrocytes.[66],[67],[68],[69]When a minimal promoter sequence from human cytomegalovirus is transfected with the GFAP in vivo, injection of the GFAP-targeted-adenovirus into C6 tumors grown in nude mice, followed by intraperitoneal GCV treatment, significantly repressed tumor growth compared with the controls.[70] Hypoxic tumor targeting New therapy targeting the hypoxic fraction of tumors is very useful as this population of cells is the most resistant to radio- and chemotherapies. Hypoxia-inducible factor (HIF) mediates transcriptional responses to hypoxia by binding to hypoxia-responsive elements (HRE) in target genes. A hypoxia/HIF-dependent replicative adenovirus (HYPR-Ad) was developed in order to target hypoxic cells. HYPR-Ad have shown hypoxia-dependent tumoral cell expression and conditional cytolysis of hypoxic, but not normoxic cells.[71] This is evidence that an attenuated oncolytic adenovirus that selectively lyses cells under hypoxia can be generated. Although this approach needs more experimental studies, the results suggest that it could be used to treat solid tumors that develop hypoxia, including the category of more malignant gliomas.Herpes simplex virus-1 Herpes simplex-virus-1 (HSV-1) has been one of the earliest recombinant vectors to be investigated in the context of cancer gene therapy. Experiments in cell culture and in animal brain tumor models have demonstrated the feasibility of HSV-1-mediated gene transduction and the killing of glioma cells by toxicity-generating transgenes. The HSV-1 vectors are particularly useful because they can be genetically engineered to replicate and spread highly selectively in dividing tumor cells and can also express multiple foreign transgenes. Intravenous gene transfer using recombinant retroviruses like HSV-1 tends to suffer from a low infectious viral titer when conducted in vivo. This is, in part, caused by the complement-mediated proteolytic inactivation of the virus in human serum. However, if the viruses are directly injected into the brain, they might not be inactivated.The HSV-1 vectors have been recently utilized as oncolytic vectors instead of replication-defective vectors [Figure - 5]. The oncolytic HSV-1 have demonstrated cytopathic effect in rat′s glioma models without damaging normal tissues [Figure - 3], providing amplified gene delivery within the tumor, and inducing specific anti-tumor immunity. Different approaches are currently undertaken to improve the efficacy of oncolytic HSV-1 therapy which include: development of new generation vectors via further genetic engineering of existing safe vectors, combination with immune gene therapy, and combination with conventional therapies.[72] Other viruses Other viral vectors, like parvovirus, hemagglutinating virus of Japan, Semliki forest virus, Measles virus, Epstein-Barr virus, Newcastle disease virus, Mumps virus, Vesicular Stomatitis virus, Influenza virus, Reovirus and Poliovirus have been tested in genetic therapy experiments in vivo and in vitro.[73],[74],[75],[76],[77] However, they lack more investigation of their specific role in glioma therapy.Clinical trials In malignant glioma, standard gene therapy approaches employing non-replicating virus vectors failed to demonstrate significant benefit in clinical studies. Therapy with oncolytic viruses seems to hold more promise in early clinical trials than gene therapy with non-replicating virus vectors.[78],[79],[80],[81] The most studied candidates for gene therapy, which are in advanced stages of clinical trials include: the prodrug activating system herpes simplex thymidine kinase (HSVtk)/ganciclovir (GCV), utilizing either retrovirus vector producer cells or adenovirus vectors; the adenovirus-mediated p53 gene transfer; the adenovirus-mediated IFN-beta gene transfer and studies with oncolytic therapy with herpes virus or adenovirus vectors. The other vectors and genes previously discussed are still in cell or animal protocols investigation stage.[82],[83] There is an ongoing Phase I/II clinical study in adult patients with recurrent GBM which is aimed at evaluating biological safety, maximum tolerated dose, and anti-tumor efficacy of a cytokine vaccination model, using a genetically modified replication-disabled Semliki forest virus vector (SFV) carrying the human interleukin 12 (IL-12) gene and encapsulated in cationic liposomes (LSFV-IL12).[84] Several other Phase I and II clinical studies in patients with recurrent malignant glioma have shown a favorable safety profile and some efficacy of retroviruses (RV)-mediated gene therapy.[85] More than 300 patients with glioma have already been treated in clinical trials with oncolytic viruses, and in most cases, the virus was administered directly into the tumor. On the other hand, a prospective randomized Phase III clinical study of retroviral (RV) gene therapy in primary malignant glioma failed to demonstrate significant extension of the progression-free or overall survival times in RV-treated patients.[86] The failure of this RV gene therapy study may be due to the low tumor cell transduction rate observed in vivo. Biological effects of the treatment may heavily depend on the choice of transgene/prodrug system and on the vector delivery methods. RV clinical trials in malignant glioma have, nevertheless, produced a substantial amount of data and have contributed towards the identification of serious shortcomings of the non-replicating virus vector gene therapy strategy. New types of therapeutic virus vector systems are currently being designed, and new clinical protocols are being created based on the lessons learned from the RV gene therapy trials in patients with malignant brain tumors. The long-term consequences of adenovirus-mediated conditional cytotoxic gene therapy for gliomas remain uncharacterized. Some studies reported detection of active brain inflammation 3 months after successful inhibition of syngeneic glioma growth. The inflammatory infiltrate consisted of activated macrophages/microglia and astrocytes, and T lymphocytes positive for leucosyalin, CD3 and CD8, and included secondary demyelination. Thus, patient evaluation and the design of clinical trials in ongoing and future gene therapy for brain glioblastoma must address not only tumor-killing efficiency, but also long-term active brain inflammation, loss of myelin fibers and persistent transgene expression.[87] Conclusions With the present results, it is clear that gene therapy strategies for gliomas
are quite promising but more critical research is required, mainly in the vector
field. Although much effort has been put into this area of research, neuro-oncologists
are still waiting for a vector system allowing for selective and efficient
tumor cell transduction. Further major advancements in virus designs, application
modalities,
and understanding of the interactions of the host′s immune system with
the virus, are clearly needed before oncolytic virus therapy of malignant brain
tumors can be introduced to clinical practice. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05003f3.jpg] [ni05003f1.jpg] [ni05003f2.jpg] [ni05003f5.jpg] [ni05003t2.jpg] [ni05003f4.jpg] [ni05003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
![[Figure - 2]](/showimage?ni/photo/ni05003f2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}