 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
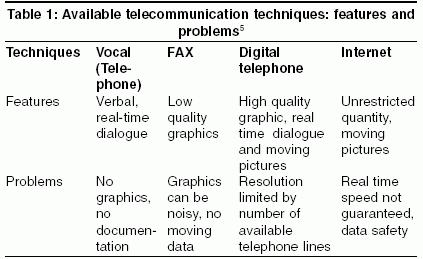
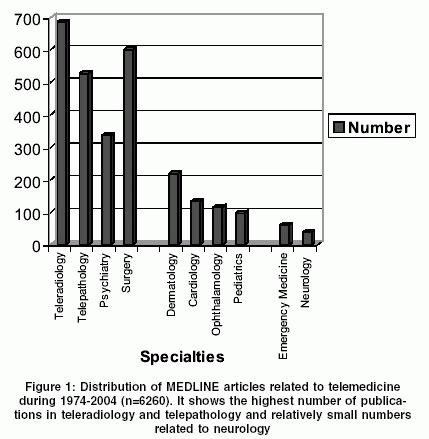
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 27-31 Review Article Telemedicine in neurology: Underutilized potential Misra UK, Kalita J, Mishra SK, Yadav RK Departments of Neurology, Sanjay Gandhi PGIMS, Lucknow Code Number: ni05004 Abstract Advances in telecommunication which started with telephone lines, FAX, integrated service digital network (ISDN) lines and now internet have provided an unprecedented opportunity for transfer of knowledge and sharing of information. The information can be used for overlapping applications in patient care, teaching and research. In medicine there is increasing utilization of telemedicine; radiology and pathology being regarded as mature specialties and emergency medicine as maturing specialties compared to other evolving specialties which include psychiatry, dermatology, cardiology and ophthalmology. Of the emergencies, status epilepticus and stroke have high potential for improving patient management. Administration of tPA was more frequent when carried out under telemedicine guidance. Telemedicine has great potential for medical education. The principles of education are in congruence with those of telemedicine and can be closely integrated in the existing medical education system. Our experience of telemedicine as a medical education tool is based on video conferencing with SCB Medical College, Cuttack. We had 30 sessions during 2001 to 2004 in which 2-3 cases were discussed in each session. The patients' details, radiological and neurophysiological findings could be successfully transmitted. These conferences improved the knowledge of participants, provided an opportunity for a second opinion as well as modified the treatment decisions in some cases. The advances in telemedicine should be utilized more extensively in neurology, especially in emergency management, epilepsy and stroke patients as well, as it may have a role in neurophysiology and movement disorders. Key Words: Telemedicine, stroke, epilepsy, patient care, neurology, menigitis, movement disorder Introduction Rapid expansion in information technology has affected all aspects of modern society including industry, commerce, banking, education and entertainment. Increasing cost and inequitable access to quality healthcare has created the need for information technology transferring patient-related information. Telemedicine has created enormous opportunities for development in terms of improved efficacy and productivity. Telemedicine has provided unprecedented access to information and various sources in the context of health.[1]Telemedicine is closely related to telecommunication. It has been defined as delivery of healthcare services to the underserved, employing telecommunication.[2] Telemedicine uses advanced telecommunication for transferring patient′s data for making diagnosis, improving disease management in remote areas and conducting research.[3] The underlying principle is transfer of information, which may be applied to any of the intended areas of medicine, patient care, teaching and research. History: The history of telemedicine can be categorized into 3 major periods; each related to significant advance in information technology, telecommunication and computers. The first telecommunication era, which spanned the 1970s and 1980s, depended on broadcast and television technology, which were cumbersome, complex and often unavailable communication systems. Digitization of telecommunication and computer advances ushered the second digital era in the late 1980s. This included integration of telecommunication and computer processing coupled with a relatively large amount of information on limited bandwidth. The integrated service digital network (ISDN) technology permits simultaneous transmission of voice, video and biomedical data at relatively high speed within a ′universal′ network. With further developments, the era of digital communication is being challenged and replaced by the Internet era. The interest in the Internet as a telemedicine tool is at least in part due to the frustrations of telemedicine users with the inability to provide accurate and timely information at an affordable price.[4] The problems related to the Internet in telemedicine have already created considerable interest in the Next Generation Internet (NGI) or Internet 2(1-2). Technical aspects: Telecommunication has been usually restricted to the use of telephone lines. [Table - 1] summarizes the presently available different standards of line connections together with their characteristics and shortcomings. A normal telephone allows vocal communication, has the advantage of real time dialogue but neither graphic nor print can be transmitted and the results of communication are not automatically documented. Integrated service digital network (ISDN) allows greatly enhanced quality including graphics and moving pictures. The transmission rate and resolution quality is limited by the number of available lines; the advantage is that the data transfer occurs at a constant rate once the lines have been activated. The transmission rate is constant at 57 KB/S for a standard telephone line and 128 KB/S for ISDN, whereas for Internet it is not fixed, depends on the type of physical connection and the degree of occupation of the net and therefore is unpredictable. Transmission time for a sequences of six MRI scans (40 MB) is 10 min, a 10-min recording of 64-channel EEG takes about 12 min and to send a 3-min video of low quality (MPEG1) consumes 16 min and of good quality (MPEG2) more than 1 hour of transmission time.[5] Present status: A MEDLINE search with the key word ′telemedicine′ revealed more than 6373 articles and only 11 were found with key words epilepsy -telecommunication/ telemedicine. Epilepsy is the commonest neurological disorder and may be a surrogate marker of the use of telemedicine in neurology. The number of MEDLINE entries containing key words does not yield the exact number of scientific studies conducted but does provide a basis for comparison. More than 6373 articles contained the term telemedicine or telecommunication. The leading numbers of articles were in radiology (686), pathology (528), surgery (601), dermatology (218) and cardiology (133). Other fields were less common such as psychiatry (336), pediatrics (96), pregnancy (40), neurology (39), neurosurgery (20) and sleep (5) [Figure - 1]. The leading fields of radiology and pathology correspond to the number of queries of investigative techniques. The term imaging was found in 274, video in 170, and electrocardiography in 14. EEG, the typical investigation of epilepsy was found in 4 papers only. The most commonly mentioned aim of telemedicine was education (371), followed by diagnosis (280), consultation (240), and therapy (122). Other indications were instrumentation (206), legal problems (99), costs (90), and payment (27).[5] The clinical telemedicine applications have been considered on two axes: the vertical axis represents the level of maturity of application. These attributes include technical feasibility, diagnostic accuracy, sensitivity, specificity, clinical outcome and cost-effectiveness. Teleradiology and telepathology rank high on the maturity scale. Psychiatry, dermatology and ophthalmology are regarded as maturing specialties whereas surgery, pediatrics, emergency medicine and rare diseases are emerging specialties with respect to telemedicine applications.[6] The use of telemedicine has been increasing but the rise has been steep since 1994. There was a slight increase from 30 to 70 articles in the period between 1984-1991, a similar increase occurred in 1992 but a non-linear, much larger increase exceeding 300 /year occurred in the year 1994. This increase was not due to an increase in the number of MEDLINE articles, which increased moderately from 300,000 to 400,000 per year. During this period, the growth of articles in telemedicine contrasts with a less impressive increase in neurology and epilepsy. In neurology, telemedicine has the greatest potential in the management of emergencies such as status epilepticus, stroke and subspecialties such as movement disorders and neurophysiology. Epilepsy: Epileptic seizures can be infrequent and difficult to diagnose. The best way to diagnose them is by observation of the seizure and in its absence one has to rely on the description of a bystander. The data concerning seizures are so important that all parts of the information should made available to the physician so as to make or revise the diagnosis. Epileptic patients with multiple handicaps have limitations of traveling for consultation and investigations, which may involve different centers and sometimes the investigations may have to be repeated. Communications between different hospitals and physicians in difficult-to-diagnose epilepsies can be greatly helped by telecommunication. This would not only avoid frequent and sometimes arduous visits to experts in different hospitals and repeated investigations but also allow simultaneous opinion of different physicians or experts. Status epilepticus is a neurological emergency; often a patient is admitted to a primary center and is referred to another hospital or a specialized center when the seizure is not controlled. When the patient reaches a specialized center he may be undergoing status epilepticus for several hours or even more than a day. This results in several complications and poor prognosis. Early diagnosis and prompt treatment would go a long way in controlling the attack and improving the prognosis. Telemedicine and acute stroke: In ischemic stroke, recombinant tissue plasminogen activator (rtPA) is a major breakthrough and if administered within 3 hours of onset of stroke it results in improved survival and outcome.[7] Many institutes lack the resources and specialized team providing fulltime response to acute stroke patients. These institutes depend on the rapid transfer of patients to nearby regional stroke centers for therapy. The primary reason for patients not receiving this therapy is late arrival after the 3 hours of window period. Telemedicine is emerging as a time-saving efficient means. In the University of Maryland Medical center, employing a pair tilt and zoom camera with remote site control allowing 2-way real time audiovisual communication and CT image transfer, 50 strokes consultations between 1999 and 2001 were reviewed. Of these, 23 were managed through telemedicine linkage and 27 by traditional telephone conversation followed by transfer. Of the 23 telemedicine consultations, 2 were aborted because of technical difficulties. Of the patients evaluated by the traditional method 3.8% (1/27) received rtPA whereas 23.8% (5/21) in the telemedicine group received rtPA and there were no complications of this therapy. Telemedicine provided a treatment option not previously available at a remote hospital. For the administration of rtPA, telemedicine was safe, feasible and was well received.[8] Assessing the stroke patients and their CT scan by using a conventional videoconference system offers an opportunity to improve stroke care in remote and rural areas. In a study from Swabia seven rural hospital were connected to the stroke unit with the use of videoconference link. One hundred and fifty-three patients were examined by teleconsultation and a relevant contribution could be made in more than 75% cases regarding diagnostic workup, CT assessment and therapeutic recommendations.[9] Although the number of emergencies is increasing, there is growing anxiety about medical errors and the increasing number of medical negligence cases. Pre-hospital use of telemedicine for stroke is already being piloted, linking patients in an ambulance to the emergency department. Telemedicine in neurological outpatients′ service: In remote areas where neurologists are not available, telemedicine has been used for providing outpatient consultation to neurological patients. In a randomized controlled trial the efficacy of telemedicine consultation was compared with face-to-face consultation, the groups comprising 82 and 86 patients respectively. The diagnostic categories were similar in the two groups. The patients in the telemedicine group had more investigations but there was no difference in the number of drugs prescribed. The patients were generally satisfied with both the processes though they were concerned about confidentiality and embarrassment in the telemedicine consultation. Telemedicine though feasible in the OPD setting is less well accepted than face-to-face consultation and leads to over-investigations.[10] However, in a remote area where the number of neurologists is too low, telemedicine may become a viable option, especially in the developing countries. Medical Education Telemedicine has great potential to transform medical education at the undergraduate, postgraduate and professional levels. The educator has to select the appropriate context, content, effective methods and efficient delivery to suit the needs of the largest number of learners. In medicine, education has to continue throughout the professional life. Learning is maximal when adults act as self-directed motivated learners, perusing the topics of their interest in an appropriate context i.e. interactive, practical and self-paced.[11] These principles can be incorporated into technology-mediated distant education programmes.[12] Internet has provided further opportunities at low cost and has the ability to support complex multimedia presentations to augment learning. Internet has created learning communities. Online CME and web-based CME have also provided CME credits for practicing physicians.Our experience with video conferencing for Neurology teaching in India Need-based neurology educational teleconferencing between Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow and SCB Medical College, Cuttack which are 1500 km apart was conducted. Faculty members and residents of the two departments participated. Desktop video conferencing system with PTZ camera, communication link 126 KBPS ISD telephone line were employed during 2001-2004. There were 30 sessions, 22 of which were successful and 8 partly successful due to power and communication failure. In each session 2-3 cases were discussed and clinical pictures, neurophysiological and radiological data were illustrated. Discussions provided inputs for both learning as well as patient management.[13] A need of extending these sessions to other institutes in the country, and to specialty groups in other areas of neurology such as emergency neurology, neurophysiology and movement disorders has been felt.In the available literature we could get only a few reports from India in which telemedicine was successfully employed. The Mahakumbh Mela, a religious congregation, occurs every 6 and 12 years in which millions of religious Hindus gather for religious ceremonies, preaching and discussions. Such a large gathering of people is associated with inherent health problems such as infections and accidents etc. Providing health care to the Kumbh attendees is a major public health problem. The Sanjay Gandhi Post Graduate Institute took the initiative of providing telehealth care for evading cholera outbreak in the Mahakumbh Mela, Allahabad, UP.[14] Ganapathy from Chennai took the initiative of providing consultation to distant areas in India in Aragonda and Sriharikota. They also have connectivity with remote areas of Northeast India as well.[15] Desai et al used telemedicine consultation between a tertiary cancer center and a rural cancer hospital. Ninety-three cases were analyzed in which static and telepathology was used to obtain a consultation between Tata Memorial Hospital, Mumbai and Nargis Dutt Memorial cancer hospital at Barshi, a rural area. A diagnosis was offered in 92 cases (98%).[16] Is it only the numbers which matter? In developing countries, increasing population and a very low doctor-patient ratio is a difficult challenge. About 750 neurologists in a country with a population of 1 billion is very inadequate and it will take more than 20 years to achieve a ratio of one neurologist per 50,000 population at the rate of 50 neurologists produced per year; but it is not only the number which is important. Increasing specialization has reduced the number of physicians who are good at managing emergencies. Although the number of emergencies is increasing, there is growing anxiety about medical errors and the increasing number of medical negligence cases.There is no single solution for upgrading the emergency services; but a favored model has been a large central hospital with associated local hospitals to which patients are discharged; but it may make the services worse rather than better. Medical emergencies usually occur in a patient′s home and are followed by a journey to the hospital, assessment, admission, treatment and then discharge. A large central hospital means a long journey, which may delay treatment and influence the outcome as in status epilepticus, stroke etc. In India the road and transportation are far from satisfactory. Increased distance also causes a problem for visiting families and weakens the link with primary care, which is crucial for discharging the patients. A large number of patients in large emergencies lead to long waiting periods, usually in a trolley. The local hospitals do not share care or staff with a large hospital and have poor nursing and medical infrastructure and are uncomfortable managing serious patients. They thus assume the role of nursing homes rather than hospitals. Black has proposed a reversing model in which patients are admitted to a local hospital, which would be an assessment area of the big hospital. The medical and nursing staff would be part of the team working in the central hospital and would rotate between the hospitals. The local unit would have imaging (CT) and laboratory (EEG, ECG, biochemistry) support and high-quality electronic links with the central hospital that would allow the specialist to know almost as much about the patients as if they were examining them directly. Such a system would result in avoiding delay in treatment. Those who don′t need admission could be quickly discharged, maybe within one day, and some patients would not need to go to the central hospital; those who go to the central hospital would not need to be assessed again, the transfer and admission would be faster.[17] Cost-effectiveness: The cost-effectiveness of telemedicine has been a concern because in a study from the UK, comparison of 65 patients in a conventional group and 76 in a teleconsultation group revealed that the telemedicine group needed more investigations and reviews than the conventional group. The average cost of conventional consultation was 49 pounds sterling compared to 72 pounds sterling for the telemedicine group.[18] Legal questions: Application of telemedicine has raised several legal questions. Data security being the most important and accidental loss and occurrence of faults must be prevented by providing effective data control management and artefact recognition. As personal data are involved, the possibility of intended or criminal abuse must be taken into account and prevented. Special encryption mechanisms that secure data against unauthorized access and even modification are therefore necessary.[19] Patients′ rights to confidentiality are paramount. Unless the regulation for special situations has been agreed upon by both sides, the liability is on the side of the consulting rather than advising physician. Procedures for reimbursement of logistic costs or payment offers need to be developed. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05004f1.jpg] [ni05004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}