 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
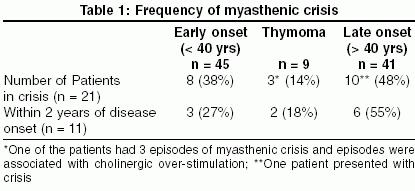
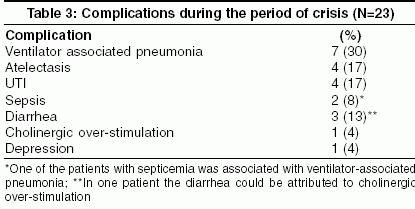
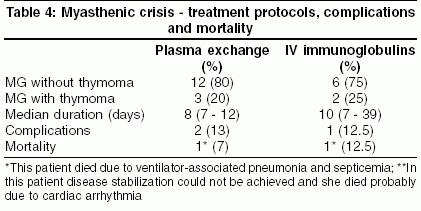
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 37-40 Original Article Myasthenic crisis: Clinical features, complications and mortality Murthy JMK, Meena AK, Chowdary GVS, Naryanan JaishreeT Department of Neurology, The Institute of Neurological Sciences, Care Hospital, Hyderabad Code Number: ni05007 Abstract BACKGROUND AND OBJECTIVE: Myasthenic crisis is a life-threatening complication of myasthenia gravis (MG) and when treated aggressively is associated with good outcome. Key Words: Myasthenia crisis, plasma exchange, intravenous immunoglobulins, mechanical ventilation Myasthenia gravis (MG) an autoimmune disorder of the neuromuscular junction tends to be characterized by exacerbations and remissions. Myasthenic crisis is a serious complication of MG and is defined as weakness from acquired MG that is severe enough to require intubation,[1] a situation that corresponds to Class V of the Myasthenia Gravis Foundation of America (MGFA) classification.[2] MGFA considers the most severely affected muscle to define the patient′s Class and avoided defining "myasthenic crisis". Class IV and Class V of MGFA clinical classification correspond to severe myasthenia. Myasthenic crisis may complicate in 15 to 20% of patients with MG.[3],[4] Materials and Methods We retrospectively identified all the patients with episodes of myasthenic crisis from the case records of the patients with myasthenia gravis seen by the senior author. Diagnosis of MG was established by neostigmine test and decrement response. Myasthenic crisis was defined as weakness from acquired MG that is severe enough to require intubation.[1] Patients with perioperative respiratory crisis associated with thymectomy were not included. Results Of the 95 patients with MG including 9 patients with thymoma seen by the senior author, 21 (22%) patients had 23 episodes of myasthenic crisis. Median age at the onset of crisis was 40 years (range 28-75 yrs) and the ratio of men to women was 1.3:1. The crisis episodes occurred within 2 years (range 9-24 months) of disease onset in 11 (52%) patients. Thymoma was present in 14% (3/21) of patients with crisis, on the other hand 3 (33.3%) of the 9 patients with thymoma developed crisis; one of them had 3 crisis episodes. This patient also had associated cholinergic over-stimulation [Table - 1].Weakness involved the respiratory, oropharyngeal, and neck muscles in 95% of the patients at the time of intubation. All patients had generalized weakness in addition. Infections were the most common primary precipitants of crisis occurring in 65% of patients and in one patient it was related to poor drug compliance [Table - 2]. The median duration of the crisis episode was 11 days (range 7-39 days), and median NICU stay was 15 days (range 9-47 days). One patient who needed assisted ventilation had severe depression. Whenever an attempt was made to wean him off the ventilator he used to get panic attacks. During these episodes he used to hyperventilate and get exhausted resulting in low tidal volume. All the patients were managed on SIMV ventilator mode. Cholinergic medication was stopped during the period of mechanical ventilation. Hospital acquired infections were the common complications. Ventilator-associated pneumonia (30%) was the commonest infection [Table - 3]. Fifteen (65%) episodes were treated with small volume PE and 8 (35%) episodes received IVIg. The outcome was similar with both the treatment modalities. In none of the patients were the treatments stopped prematurely. The time taken for the disease to stabilize, the median number of days for extubation, was 8 days (range 7-12) in the PE group and 10 days (range 7-39) in the IVIg group. Disease stabilization could not be achieved in one patient in the IVIg group [Table - 4]. Two patients in the PE group developed hypotension during one of the exchange schedules. This could be corrected with volume expansion. One patient in the IVIg group developed elevation in blood urea and serum creatinine after four doses of IVIg. However he was given the fifth dose without any adverse events. With conservative treatment urea creatinine levels became normal. Two (8%) of the 23 episodes of crisis were fatal, one resulted from ventilator- associated pneumonia and septicemia, the other was related to crisis. In this patient disease stabilization could not be achieved with IVIg; while she was on T-piece trial, she had sudden cardiac arrest, probably related to cardiac arrhythmia, from which she could not be revived. All the 19 patients who survived to discharge had complete resolution of admission symptoms. All patients were started on steroids before discharge. Discussion Myasthenic crisis frequently occurs within the first 2 years after disease onset,[3] and about one-fifth of the patients develop crisis episodes within the first year.[9] Most often myasthenic crisis develops in patients with generalized myasthenia. Rarely, some patients may experience respiratory failure without generalized weakness.[10] A third of the patients who survive the first crisis experience a second crisis. Myasthenic crisis is more common in patients of myasthenia gravis associated with thymoma.[3],[4] A cholinergic crisis is less common and a combination of both crises is often clinically encountered.[4] All the three episodes of myasthenic crisis in one of the patients with thymoma were associated with cholinergic overstimulation. Infections are the most common precipitating factors, 30-40% of cases. Several drugs which affect the neuromuscular junction are also associated with myasthenic crisis.[1],[4] However; no risk factors are identified in 30 to 40% of patients with myasthenic crisis.[4]Early intubation and mechanical ventilation is perhaps the most important step in the management of myasthenic crisis. This can be achieved by instituting assist-control (AC) or SIMV. Although large tidal volumes have been recommended,[4] more recent literature defends that smaller tidal volumes (7-8 mL/kg) with faster respiratory rates (12-16 breaths/min) should be used to avoid lung injury adding intermittent sighs (1.5 x tidal volume, 3 to 4 times every hour) to avoid atelectasis.[3] Nomori and Ishihara[11] have managed five patients with MG with pressure-controlled ventilation via a mini-tracheotomy tube (MTT). The MG patients could be converted from conventional volume-controlled ventilation to pressure-controlled ventilation (PCV) via MTT. Clinically, PCV via MTT achieved adequate ventilation without impairing their speech. Non-invasive bi-level positive pressure ventilation (BiPAP) has also been used successfully in patients with respiratory failure caused by myasthenic crisis. This study suggests BiPAP may prevent intubation in patients with myasthenic crisis. Eleven episodes of crisis in 9 patients were initially managed with BiPAP and endotracheal intubation was avoided in 7 of these 11 trials. The presence of hypercapna with PaCO2 > 50 mmHg at onset predicted BiPAP failure and subsequent intubation.[12] Most patients require ventilation for a brief period, less than two weeks.[3],[13] In the series by Thomas and colleagues,[3] half of the patients were extubated by 13 days, and 75% by 31 days. In this study a pre-intubation serum bicarbonate level >30 mg/dl, a post-intubation vital capacity of <25 ml/kg on day 3 or later; and age >50 years have been shown to be independent predictors of prolonged crisis. These clinical variables may serve as clinically useful criteria for estimating the need for mechanical ventilation beyond two weeks. Atelectasis, and ventilator-associated pneumonia are the common complications of prolonged mechanical ventilation.[3],[14] Plasma exchange and intravenous immunoglobulin are the two immune-directed treatments used for patients with actual or impending myasthenic crisis. Studies comparing PE with IVIg have demonstrated equal efficacy but significantly fewer and less severe side effects for the IVIg treatment. Improvement usually begins within a few days of treatment.[15],[16] Studies of daily PE compared with every other day exchange have demonstrated no statistically significant improvement in the strength or number of days of mechanical ventilation but have shown a trend towards improved strength at the end of therapy without increased side effects.[17] However, in a retrospective study PE (compared with IVIg) was associated with a superior ventilatory status at 2 weeks and one-month functional outcome. However, the complication rate was higher with PE.[18] Our study had also demonstrated equal efficacy of both treatments and in the IVIg group disease stabilization could not be achieved in one patient who died. We gave small-volume PE. For patients with severe crisis, more than one course of PE or IVIg may be necessary. A retrospective analysis showed the failure rate of one course of IVIg treatment to be 20%.[18] Advancement in the critical care techniques and the introduction of immunomodulation therapy have dramatically reduced the mortality rates of myasthenic crisis. A recent study suggests that aggressive respiratory treatment (use of suction, intermittent positive pressure breathing or bronchodilator treatments, sighs, and chest physiotherapy) can lower the risk for atelectasis and ventilotor-associated pneuomonia.[14] Before 1955, myasthenic crisis was fatal in 80% of episodes.[19],[20] In the recent Columbia series the mortality rate was 10% overall, half of those dying after extubation.[3] In the Columbia series all deaths were attributable to severe medical comorbidity. The mortality in our series was 9.5% and one of the deaths was probably related to cardiac arrhythmias. Cardiac arrhythmias occur in up to 17% of patients with myasthenic crisis.[21],[22],[23] Certain limitations of our study must be acknowledged. This was a retrospective study and had a limitation of available clinical data. The treatment allocation between PE and IVIg was not randomized and was based on the accessibility to PE services and affordability to the patients. In spite of such limitations this series suggests that both PE and IVIg are equally effective and safe. To achieve good outcomes all efforts should be directed at decreasing the duration of intubation and also aggressively treating the associated medical comorbidity and complications. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05007t2.jpg] [ni05007t4.jpg] [ni05007t1.jpg] [ni05007t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}