 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
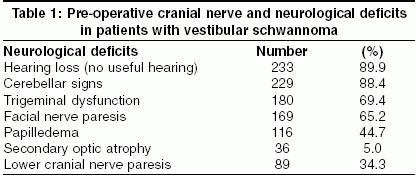
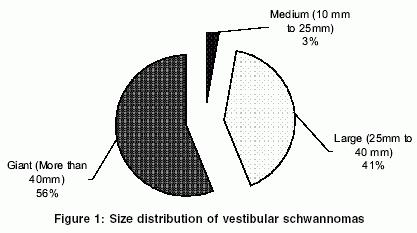
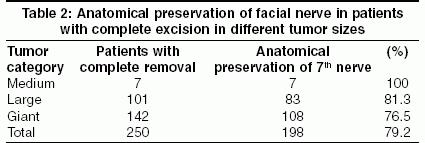
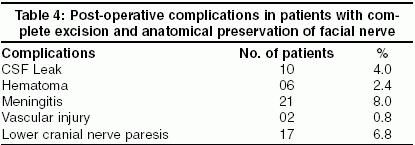
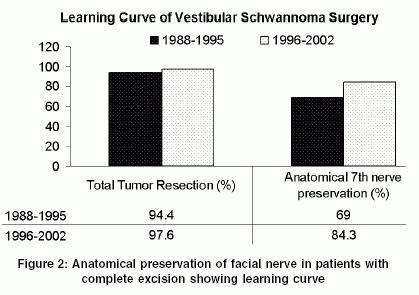
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 41-45 Original Article Surgery of vestibular schwannomas: An institutional experience Jain VijendraK, Mehrotra Naveen, Sahu RabiNarayan, Behari Sanjay, Banerji Deepu, Chhabra DevendraK Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow Code Number: ni05009 Abstract AIMS: To report management results of vestibular schwannomas (VS) treated surgically in our institute, with particular reference to completeness of tumor excision, facial nerve and hearing preservation and complications of surgery. Key Words: Vestibular Schwannomas, cerebello-pontine angle, retro-mastoid approach, facial nerve perservation Introduction There are only a few reports discussing the management consideration in vestibular schwannomas (VS) from India.[1],[2],[3],[4] To quote Ramamurthi, saving life and functions of the lower cranial nerves still forms the main goal in majority of patients who come with large tumors.[5] We report the results of management of vestibular schwannomas in our institute.Materials and Methods Two hundred and sixty-five patients with VS were treated in our Institute from 1988 to December 2002. Six cases were excluded from the study as in three elderly patients only a ventriculo-peritoneal shunt was performed and three patients who had tumor recurrence after surgery in another hospital. Thus, 259 patients included in this study, had their surgery done for the first time at our institute. In 9 patients complete excision of the tumor was not achieved, as part of the tumor capsule was adherent firmly, either to the brainstem or to the facial nerve and could not be safely dissected. Thus the surgical outcome of complete excision of VS was studied in 250 patients.The clinical records of the patients were reviewed; the facial nerve function was graded according to House-Brackmann [HB6] score pre-operatively, post-operatively, at the time of discharge and at follow up. Pre-operative pure tone audiometry was done in all patients to assess the degree of hearing loss. Criteria for useful hearing was taken as hearing loss <60 decibel (Norstadt Classification for audiometric hearing).[7] Post-operative hearing assessment was done only in those patients who had useful hearing preoperatively. The speech discrimination test was not done. The tumor size was measured (in CT and/or MRI scan) in three axes that is diameter parallel to the petrous ridge, perpendicular to the petrous ridge or the vertical diameter in the coronal slices. The size of the VS was taken as the largest diameter in any one of these three axes. The tumors were then categorized according to the classification proposed by Jackler[8] et al. For patients with bilateral tumors, the side operated was considered for categorization. All the patients were operated via the retro-mastoid sub-occipital transmeatal approach in park-bench position, except for two patients who were operated in sitting position. Cavitron ultrasonic aspirator was used in a few cases. The facial nerve stimulator was not utilized. The intrameatal component of the tumor was removed and the lateral aspect of the intrameatal facial nerve defined, after drilling the roof of internal acoustic meatus (IAM). A piece of muscle was used to seal the drilled IAM in all patients. In the 3 patients during re-exploration for the persistent cerebrospinal fluid (CSF) rhinorrhea, fibrin glue with muscle patch was used to seal the drilled IAM. All the patients were followed up at 6 weeks, at 3 months, at 6 months and yearly thereafter. The maximum follow up was of 11 years. Results There were 151 males and 108 females with ages ranging from 11 to 78 years. No predilection was observed as far as side or sex were concerned. Eleven patients (4.2%) had bilateral tumors (Neurofibromatosis type-2). In one of these patients bilateral surgery was performed and complete excision of the tumor was achieved on the side with the larger tumor and a sub-total excision was done on the contralateral side after a period of time. Two of these patients had coexisting small neurofibroma arising from lower cranial nerves that was asymptomatic and was detected during surgery. These tumors were not resected.There was no useful hearing in approximately 90% patients. Varying degrees of facial nerve paresis was observed in 65.2% cases. The other symptoms were of raised intra-cranial pressure, trigeminal dysfunction and cerebellar ataxia [Table - 1]. One hundred and forty five patients (56%) had giant, 41.3% had large and 2.7% of patients had medium sized tumors [Figure - 1]. Twenty-two patients underwent ventriculo-peritoneal shunt procedure prior to the definitive surgery. Thirteen (5.2%) patients required ventriculo-peritoneal shunt surgery in the post-operative period. Complete excision of the VS along with intra-canalicular (intra-meatal) portion was achieved in 96.5% (250/259) of patients. Staged tumor resection was done in 5 patients. Out of the nine patients in whom complete excision could not be achieved; 3 patients had tumor adhered to the brainstem and in 5 patients the tumor was adhered to the facial nerve (part of the tumor was left to avoid nerve injury). In one patient, only a subtotal removal was possible due to massive intra-operative hemorrhage. Facial nerve was anatomically preserved in 79.2% (198/250) patients with complete tumor excision. Nine patients died in post-operative period, and 189 patients were analyzed for facial nerve function at time of discharge. The facial nerve preservation rates were 76.5% for giant size VS and increased rates were observed with tumors of smaller sizes (81.3% for large and 100% for medium size) [Table - 2]. Further, the functional status of the facial nerve at follow up were better in patients with relatively smaller tumors who had mild grade facial paresis (H&B Grade 1 and 2) pre-operatively [Table - 3]. Twenty-seven patients had useful hearing preoperatively. Useful hearing could be retained in 8 patients (29.6%) postoperatively. Amongst these 8 patients, 1 had giant size tumor, 4 had large tumors and 3 had medium sized tumor. Cerebrospinal fluid (CSF) leak occurred in 4% (10/250) patients. CSF rhinorrrhea and CSF otorrhea occurred in 6 and 2 patients respectively. Most cases were managed conservatively with or without lumbar puncture and CSF drainage. Three patients required re-exploration and plugging of the drilled internal auditory meatus (IAM) for CSF leak. Three patients (1.2%) developed operative site hematoma and 3 patients had an extra-dural hematoma (1.2%) and all of them underwent re-exploration surgery. Twenty patients (8.0%) developed post-operative meningitis. Eighteen patients responded to the anti-meningitic treatment. Vertebral artery injury occurred in 2 (0.8%) patients; the procedure was abandoned and one patient underwent tumor excision at a later date. Both these patients were discharged without any neurological deficit due to vertebral artery injury. Post-operative lower cranial nerve paresis developed in 17 (6.8%) patients [Table - 4]. These patients required nasogastric tube feeding and three of them required temporary tracheostomy. However the lower cranial nerve paresis improved functionally during 4-6 weeks follow-up. The mortality was in 6% patients (15/250). Massive cerebellar edema leading to brainstem failure occurred in 3 patients. Air embolism (which includes one case operated by sitting position) and meningitis were responsible for mortality in 2 patients each. Massive intra-operative haemorrhage, operative site haematoma, post-operative myocardial infarction, fulminant septicemia and severe anaphylactic reaction due to mismatched blood transfusion caused mortality in one patient each. No definite cause of death could be established in three patients who could not be revived following surgery. Discussion The last century has witnessed a considerable evolution in the management of VS with contributions from eminent neurosurgeons like Cushing who was the first to reduce mortality rates from 50% to 11%[9]. Later Walter Dandy reported complete excision with no mortality in his series of 5 patients.[9] In 1964, House[10] introduced operating microscope for trans-labyrinthine approach and a year later in 1965 Rand and Kurze[11] utilized the operating microscope for trans-meatal posterior fossa approach. With the availability of operating microscope, safe modern anesthesia and refinements in the microsurgical technique the goal of VS surgery has shifted from complete excision to excellent facial nerve function and preservation of cochlear nerve function. During the past quarter of century the advances in neuro-imaging like high resolution computed tomography and multiplanar magnetic resonance imaging have resulted in early detection of VS and an increased frequency of smaller lesions being operated.In this present study, 97% of patients had either a large or giant sized VS. Ninety percent of patients had no useful hearing at the time of presentation. In contrast to certain western literatures,[12],[13] majority of our patients sought medical attention at a stage when they developed disabling cerebellar ataxia (88.4%) and/or the symptoms of raised intra-cranial pressure. Pre-operative ventriculo-peritoneal shunt is not required in majority of the patients, but some patients report late with signs of raised intra-cranial pressure requiring emergency shunt procedures. In the present study the pre-operative shunt was done in 8 patients at our center and 14 patients had shunt done elsewhere before they were referred for definitive surgery. The incidence of preoperative shunt was as high as 66% in the series reported by Ramamurthi et al.[5] Complete tumor excision was achieved in 96.5% (250/259) of the patients. Yamakani et al,[14] reported complete tumor excision in 86% patients by retro-mastoid approach for large acoustic tumors. Lanman et al reported a higher rate (96.3%) of total removal by the trans-labrynthine approach.[13] Ebersold et al[15] achieved total tumor resection in 97.2% (249/256) by retro-mastoid approach for tumors of all sizes. Samii et al[16] have reported complete excision in 97.9% patients by sub-occipital trans-meatal approach. Anatomical preservation of facial nerve was achieved in 79.2% (198/250) patients. In the giant category facial nerve preservation was 76.5% (108/141) and in the large category was 81.3% (83/102) and 100% (7/7) for medium size tumors. In some western literatures the anatomical preservation rate is 80-90% with the removal of large tumors either by the trans-lybrinthine approach[13],[17],[18] or by the retro-mastoid approach.[12],[16],[19] Other authors have reported the anatomical preservation of the facial nerve for tumors > 4 cms ranging from 89% to 92% by trans-labyrinthine approach[20],[21],[22],[23] and 78%-94% by sub-occipital-retro-sigmoid approach[19],[23] Samii and Matthias reported preservation rate of 87% with tumor size >3 cm until 1988, but in most recent 200 cases preservation rates rose to 94% independent of tumor size.[23] Moreover in our series after 1995 (in recent 166 cases) we have achieved facial nerve preservation rate of 84.3% observing that experience results in better outcome. The preservation rate was 69% (58/84) until 1995 and had subsequently increased to 84.3% (140/166) [Figure - 2]. This data confirms that there is a learning curve for surgery of VS. According to Whittaker et al a surgeon operating less than 12 cases per year cannot expect to get equal results of large series.[24] The size of the tumor, is one of the important factors responsible for the preservation of the facial nerve, having a reciprocal relationship i.e. larger the size of tumor lesser the chances of preservations[9],[13],[19] was also observed in this present study. In the present study 10.4% (27/259) patients had pre-operatively useful hearing. Post-operative hearing could be preserved in 8 of these27 patients (29.6%) in spite of their giant size in 1, large in 4 and medium in 3 patients. Though the retro-mastoid approach gives the surgeon great opportunity for saving hearing in small sized tumors, but in tumors more than 4 cm, the post-operative hearing is usually very poor as observed by Ebersold et al,[19] who reported no post-operative hearing in any of patients with tumor size more than 4 cm. According to Samii et al, patients with large tumor (30 mm x 20 mm) hearing were preserved in 23.6% (78/330).[7] Almost all authors agree that hearing preservation is more likely with smaller tumors with good pre-operative hearing.[25],[26],[27],[28],[29],[30],[31] Whittaker and Luetje are of the opinion that hearing preservation attempts should be made for tumors below 2 cm in diameter with the patient fully informed. By fully informed means that the patient understands that some hearing may be preserved in 30%-50% of cases (depending on tumor size), and that 30% of this number will have unexplained deterioration later, leaving some permanent hearing impairment; and probably only 7% to 9% of the total group will find hearing useful.[24] This delayed worsening of preserved hearing was observed by Goel et al.[32] The reported incidence of cerebrospinal fluid leak ranges between 0% and 30%, with the average approximately 12%, although making comparisons between published series is difficult because of the various methods and reporting criteria used by different authors.[33] In the present study 4% (10/250) of patients had cerebrospinal fluid leak with 3 patients requiring surgical repair and the incidence is at par with the series published by Yamakani I et al,[14] recently. However the incidence of associated meningitis in our study is slightly more (8%) as compared to some of the recent series (between 3.7 to 9.2%)[13],[17],[18],[22],[34] Although loss of cochlear and seventh nerve function are two of the major cranial nerves injuries that can occur during the surgery, there are risks of injury to lower cranial nerves in large and giant sized tumors, which can complicate the post-operative course. Judicious use of nasogastric tube feeding and planned tracheostomy can avoid major respiratory complications post-operatively. The incidence of lower cranial nerve paresis has been reported to range from 1.5% to 5.5%[8],[13],[16],[19] against 6.8% in the present study. In the present study, all the cases were operated by retro-sigmoid approach with park-bench position, except in 2 patients with sitting position. This concludes the fact that the retro-sigmoid approach in experienced hands is a good option; with good results compared to other series irrespective of the tumor size. This is an extension to the view put forward by Samii et al that from any of the available approaches, such as the sub-occipital, the middle fossa, and the trans-labyrinthine; surgeons can develop expertise to high standards, by training and experience, with respect to the optimum patient′s safety, mortality and morbidity.[16] Gormley and Sekhar et al[9] used the combined transpetrosal and retrosigmoid approach for tumors greater or more than 4 cm in the cerebello-pontine angle, especially when they extend up to the tentorial notch, because the combination allows good visualization of tumor-brain stem interface and the tentorial notch and better facial nerve outcome for these group of tumors. But in our series, using retro-sigmoid approach alone visualization of tumor-brainstem interface and facial nerve preservation could be possible in giant sized tumors with out much difficulty. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05009t1.jpg] [ni05009t3.jpg] [ni05009t2.jpg] [ni05009f1.jpg] [ni05009f2.jpg] [ni05009t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
![[Table - 3]](/showimage?ni/photo/ni05009t3.jpg){kind=link}
{kind=link}
{kind=link}