 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
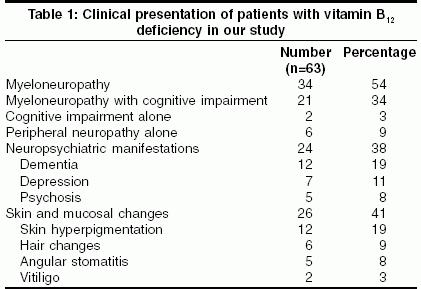
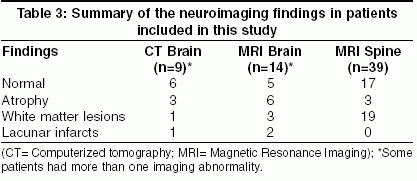
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 55-58 Original Article Clinical and laboratory features and response to treatment in patients presenting with vitamin B12 deficiency-related neurological syndromes Aaron S, Kumar Sudhir, Vijayan J, Jacob J, Alexander M, Gnanamuthu C Neurology Unit, Department of Neurological Sciences, Christian Medical College, Vellore, Tamil Nadu Code Number: ni05014 Abstract AIMS AND OBJECTIVES: To study the clinical and laboratory features of patients admitted with vitamin B12 deficiency-related (B12def) neurological syndromes. Key Words: Bone marrow smear, Vitamin B12 dificiency, Myeloneuropathy Introduction Vitamin B12 deficiency (B12def) leads to myriad neurological manifestations and affects all age groups.[1] Early recognition of this condition is essential, as it is reversible and preventable.[2] However, a significant diagnostic delay still occurs in many cases. Though there is much debate regarding the appropriate method of diagnosing vitamin B12def, the diagnosis is often made on the basis of a low serum vitamin B12 level or megaloblastic bone marrow or both.[2],[3] There are conflicting data regarding the recovery of patients with B12def presenting with neurological involvement.[4] This study was aimed at determining the common clinical presentations and outcome with treatment of patients admitted with B12def.Materials and Methods This study was conducted in the Department of Neurological Sciences of a tertiary care teaching hospital. Retrospective and prospective descriptive study was carried out over a period of three years from June 2000 to May 2003 on consecutive patients admitted with a diagnosis of B12 def-related neurological syndromes. Data were collected regarding the demographic, clinical and laboratory features. All the patients underwent detailed general and neurological examination to identify the clinical syndromes. Patients were screened for dementia by mini-mental status examination (MMSE). The diagnosis of dementia was established on the basis of DSM-IV criteria. In addition, patients suspected to have cognitive impairment underwent a detailed assessment of various cognitive domains as per the neuropsychological proforma formulated at our department.[5] Other primary degenerative dementias were excluded as per established diagnostic criteria. The diagnosis of B[12]def was made on the basis of low serum vitamin B12 levels (<200 pg/ml) assessed by radioimmunoassay or presence of megaloblastic changes in the bone marrow smear or both.[2],[3] Appropriate electrophysiological and neuroimaging studies were also performed.Patients were treated with intramuscular B12 injections (cyanocobalamin form, Neurobion forte, Merck India) at a dose of 1000 micrograms per day for seven days and then once a week for one month and thereafter once a month long-term. They were followed up for a minimum of six months and the response to therapy was noted. Assessment included a detailed general and neurological examination. In addition, laboratory parameters, neuroimaging and electrophysiological studies were repeated as per the clinical presentation. Functional status was assessed as per Barthel′s index. Pearson′s Chi-square test was used for statistical analysis. Results Demographic DataA total of 63 patients (52 males) with a mean age of 46.2 years were studied. Majority (31, 49%) belonged to the age group of 31 to 50 years. The mean duration of symptoms at presentation was 10.3 months (range 2-28 months). The majority of patients belonged to a higher socioeconomic background (based on occupation, family assets and monthly income). Professionals and skilled workers constituted 70% of the patient population. Risk factors Predisposing factors were found in only 14 (22%) patients. History of alcohol abuse (10 patients) and chronic diarrhea (6 patients) were the common underlying factors noted. Malabsorption work-up was positive in four patients. The majority were vegetarians (60%). One patient had an ileal resection. Clinical features The common systemic features were fatigue (34%), glossitis (31%), weight loss (27%) and anorexia (22%) [Table - 1]. It was noted that those with fatigue had a lower hemoglobin level (mean 10.6 gm%, SD + 2.58) when compared to those without fatigue (mean 12.4 gm%, SD + 2.20), which was statistically significant (P=0.005). Skin and mucosal changes were seen in 26 patients, 47% of them (19% of total) had cutaneous hyperpigmentation. Other findings included hair changes (9%), angular stomatitis (8%) and vitiligo (3%). Even though hyperpigmentation was an important general examination finding, it did not correlate with duration of symptoms, severity of the megaloblastic change in the bone marrow smear, or the mean corpuscular volume (MCV). Myeloneuropathy was the commonest clinical finding in 34 (54%) patients. A combination of myeloneuropathy with cognitive impairment was seen in 21 (34%) patients. Six (9%) patients had peripheral neuropathy alone. Cognitive dysfunction as the only manifestation of B12def was noted in two (3%) patients. Neuropsychiatric manifestations were noted in 24 (38%) patients and included dementia in 19%, depressive features in 11% and psychosis in 4%. The mean MMSE score in patients with dementia was 15.5 + 7.5. All patients with dementia had memory impairment. Language impairment was the next most common finding, affecting 77% of patients. Attention and concentration were unaffected in all the patients. Disorientation to space and person was seen in 55% of patients. Poor judgment and visuospatial disorientation were seen in 43% and 37% of patients respectively. All patients had features of temporal lobe dysfunction, whereas only 75% of patients with dementia had features of frontal and/or parietal lobe dysfunction. The occurrence of dementia in patients with B12def did not correlate with duration of symptoms, or the severity of megaloblastic changes in the bone marrow smear. Laboratory features All the patients had megaloblastic changes in the bone marrow smear. Mild changes were noted in 56% while moderate and severe changes were noted in 22% each [Table - 2]. Hypersegmented neutrophils in the peripheral blood were seen in only 10 patients (16%). The mean hemoglobin was 11.3 Gm %, MCV 103.1 Fl and the serum LDH 871 U/L respectively. Eleven patients (17.5%) had both their hemoglobin and the MCV within the normal range (Hb >12 Gm% and the MCV < 98 Fl). Clinical syndromes in them included myeloneuropathy in seven, peripheral neuropathy in three and dementia in one. The serum B12 levels were low (normal 200-950 pg/ml) in 35 patients (tested in 39 patients). Serum folate level was within the normal range (3-17 ng/ml). Serum homocysteine was elevated in 13 patients (tested in 14). Anti-intrinsic factor antibody was positive in 19 (76%) and anti-parietal cell antibody was positive in 17 (68%) out of 25 patients, in whom they were tested. Upper gastrointestinal endoscopy was performed in 21 patients and showed features of atrophic gastritis in 14 (66%). Malabsorption work-up was positive in four patients. Neuroimaging and Electrophysiological Findings The neuroimaging findings are summarized in [Table - 3]. Findings of the nerve conduction studies are summarized in [Table - 4]. Visual evoked potentials showed features of optic nerve dysfunction in 16 (out of 29) patients. Brainstem auditory evoked responses were abnormal in 3 (out of 21). Somatosensory evoked responses (tested in 23 patients) showed features of cervical cord dysfunction in 14 and dorsal cord dysfunction in 17 patients. Follow-up Follow-up after a mean duration of 13.4 months (range 6-34 months) after starting therapy with parenteral B12 showed improvement in 33 (54%) patients. There was no significant change in nine (14%) and 21 (32%) were lost to follow-up. Thus, in effect, 79% (33/42) of the patients who could be evaluated after six months had shown improvement. Cognitive functions showed a significant improvement. Mean MMSE scores improved by 2.4 to a level of 17.9 + 6.4 (P<0.01; 95% Confidence Interval (CI): -3.9 to -1.6). Functional status had markedly improved in them. The ′activities of daily living score′ in the Barthel index significantly increased from a pretreatment level of 62.6 + 33.2 to 75.7 + 18.4 (P<0.01; 95% CI: -24.8 to -8.3) after the treatment. The response to the treatment was not affected by the severity of the megaloblastic changes in the bone marrow or the duration of the neurological symptoms. Discussion Even though the human body has enough vitamin B12 stores to last for up to five years, its deficiency is not uncommon. The main systems affected due to B12def are the hematological, skin and mucous membranes, and the nervous system.[6] Neurological features are attributable to pathology in the peripheral nerves, optic nerves, posterior and lateral columns of the spinal cord and brain. B12def is a classic neurological ′system-specific degeneration′ in which particular sets of neurons are affected because of their selective vulnerability. An increased prevalence of B12def has been reported in patients infected with the human immunodeficiency virus (HIV).[7] However, none of our patients had HIV infection. B12def causes a wide spectrum of neurological manifestations ranging from neural tube defects[8] to changes in cognition and behavior.[9] Many unusual manifestations have been reported in infants[10] and adults including movement disorders[11] and seizures.[12]The diagnosis in our cases was based on either a megaloblastic bone marrow or low serum vitamin B12 level or both. A megaloblastic bone marrow was taken as a definitive evidence of B12def because: (i) some patients may have received B12 supplements prior to their referral to us which can influence the serum B12 levels; (ii) in a vitamin B12-deficient state, the levels first fall in the neuronal tissues and only much later is it reflected in the serum vitamin B12 levels. Therefore, a diagnosis of B12def might be missed if we solely rely on the serum levels; (iii) the presence of megaloblasts in the bone marrow is virtually diagnostic of vitamin B12 or folate deficiency. However, a serum vitamin B12 assay is mandatory in all cases of suspected B12def. A referral bias probably may be the reason behind the higher proportion of inclusion of males (83%), and those from a higher socioeconomic background (70%) in this study. However, it could also be due to the fact that the etiology of B12 deficiency seems to be immune-mediated in a significant number of patients and an autoimmune process could affect more affluent people as well. Vegetarians constituted 60% of the study population. Earlier Indian studies have also highlighted this.[13],[14] This finding confirms that vegetarians are at a higher risk of developing B12def, which is probably corroborated by the finding that vegetarians had a statistically more severe form of megaloblastic changes in the bone marrow as compared to the non-vegetarians. Even though the classical syndrome of B12def is termed ′subacute′ combined degeneration of the cord, a wide variation is noted in the duration of symptoms at the time of presentation (2 months-28 months). The deficiency can also occur acutely following exposure to nitrous oxide.[15],[16] Fatigue was the commonest symptom in this series. B12def has been implicated in conditions where fatigue is a prominent symptom such as chronic fatigue syndrome.[17] In this study, fatigue was associated with a low hemoglobin level. Hyperpigmentation over the extremities, especially over the dorsum of the hands and feet with accentuation over the terminal phalanges and inter-phalangeal joints, associated with pigmentation of the oral mucosa is characteristic of B12def. These findings resolve with therapy.[18] Myeloneuropathy was the commonest neurological manifestation in this study. In another similar study from the West, diminished vibratory sensation and proprioception in the lower extremities were the most common objective neurological findings.[1] This difference may be due to the delayed presentation of patients to our center in this study. The median duration of symptoms in our patients was 10.3 months as compared to 4 months in the Western study. The association between neuropsychiatric disorders and B12def is well known. Dementia in our study did not correlate with either the duration of symptoms or the severity of the megaloblastic changes in the bone marrow smear. These results are similar to the findings reported by Lindenbaum et al,[19] where it was shown that the neuropsychiatric disorders due to cobalamin deficiency occurred commonly in the absence of anemia or macrocytosis. A high prevalence of low serum vitamin B12 levels, and other indicators of vitamin B12 deficiency have been reported among people with Alzheimer′s disease and older people. However, evidence of any efficacy of vitamin B12 therapy in improving the cognitive function of people with dementia and low serum B12 levels is insufficient.[20] It was interesting to note that 11 patients (17.5%) had both their hemoglobin and the MCV within the normal range. Other studies both from India and the West have reported similar findings.[19],[20],[21],[22] Wadia et al[13] had shown that hematological parameters alone are likely to miss nearly 50-70 % of the cases of B12def. They used a cut-off of Hb <11 gm% and MCV < 95 fl in their study, as compared to a slightly higher cut-off taken in this study (Hb<12 gm% and the MCV< 98 fl). After a follow-up of six months or more, 54% showed improvement. This could be higher in reality, as we assumed that all the cases that were lost to follow-up might not have improved. The response to treatment was not affected by the severity of the megaloblastic changes in the bone marrow or the duration of symptoms. This finding was contrary to the findings of Lindenbaum et al,[19] who showed that the degree of improvement over the baseline neurological status after treatment was inversely related to the duration of symptoms and hematocrit. Functional status also improved as assessed by the Barthel index. However, it should be noted that Barthel′s index may not be appropriate for assessing the outcome of varied neurological syndromes including peripheral neuropathy. This could be a limitation to generalizing the results of this study. A high index of suspicion of B12def is needed in patients presenting with myelopathy, cognitive decline, or neuropathy, especially among the pure vegetarians and the elderly. Skin changes might be an important clue towards the diagnosis. The duration of symptoms is highly variable. A normal hemoglobin and MCV, and even a normal serum B12 level does not rule out B12def; hence other tests like bone marrow smear might be useful in diagnosing this condition, as it is reversible in a majority. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05014t3.jpg] [ni05014t1.jpg] [ni05014t4.jpg] [ni05014t2.jpg] |
| |||||||||

{kind=link}
![[Table - 2]](/showimage?ni/photo/ni05014t2.jpg){kind=link}
{kind=link}
![[Table - 4]](/showimage?ni/photo/ni05014t4.jpg){kind=link}