 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 53, No. 1, January-March, 2005, pp. 90-92 Original Article Protective effects of cisternal irrigation on leptomeningeal and cortical structures in meningitis: An experimental study Aydin MehmetDumlu, Gündogdu C, Akçay F, Gursan N Departments of Neurosurgery, Ataturk University, Erzurum Code Number: ni05026 Abstract BACKGROUND: Meningitis, termed as foreign material collection in the subarachnoid space, leads to various meningeal, cerebral and spinal cord pathologies. Meningitis still remains a problematic disease with severe complications in spite of advanced medical technology.AIMS: In this study, we aimed to investigate the role of cisternal irrigation in the prevention of meningitis complications. SETTING AND STUDY DESIGN: Experimental study was done in the Social Security Hospital of Erzurum. Histopathological specimens were evaluated in the Pathology Department in the Ataturk University Research Hospital, Erzurum, Turkey. MATERIALS AND METHODS: This study was conducted on twelve lambs. Experimental meningitis was achieved with streptococcus pneumonia. Two animals were not treated. Ten animals were given CefotaximeR (4x1 g/day) for 20 days, and additionally half of these animals underwent cisternal irrigation. Then, all animals were sacrificed and brains were observed histopathologically. RESULTS: Massive purulent CSF formation, hemorrhagic cortical lesions, vascular congestion, leptomeningeal and cortical adhesions and brain edema were observed in the non-irrigated group, but these findings were observed slightly or absent in the irrigated group. CONCLUSION: Meningitis can affect all central neural tissues, consequently serious central nervous system lesions may develop. The irrigation procedure may decrease the percentage and severity of meningitis complications by way of the excretion of inflammed purulent collection from the subarachnoid spaces. Key Words: Experimental meningitis, irrigation, meningovascular changes Introduction Meningitis still remains a serious disease in spite of advanced treatment methods.[1] It causes several life-threatening complications such as ventriculitis, ependymitis, focal encephalitis, hydrocephalus, porencephaly, multicystic encephalopathy, epilepsia, mental retardation, deafness and peripheral nerve palsies.[2],[3] Materials and Methods This study was conducted on 12 lambs of 5-7 kg. All experiments were
performed according to the guidelines for the ethical treatment of
animals of the Atatürk University Research Hospital. All animals were anesthetized with 20 mg/kg of sodium penthobarbital for preoperative preparation. Thereafter, 0.2 mL/kg of the anesthetic combination (Ketamine HCL, 150 mg/1.5 mL; Xylazine HCL, 30 mg/1.5mL; and distilled water, 1mL) was subcutaneously injected before surgery. Five mL of infected soluble material containing 107/mL streptococcus pneumonia was injected into the cisterna magna of animals. Animals were followed up for 25 days. Meningitis developed in all animals within 5 days. Two animals (Group I) were not treated for observing the effects of meninigitis. Ten animals (Group II, n=5) were given Cefotaxime (4x1 g/day IV) for 20 days. Additionally, five of these animals were also given cisternal irrigation (Group III, n=5). We prepared an irrigation solution by mixing isotonic saline solution, dextrose solution (5%)
and distilled water at a ratio of 50/30/20, respectively. For irrigation,
a 3F catheter was permanently inserted into the cisterna magna through
the foramen magnum and the other 3F catheter was permanently placed
in the subarachnoid space at the lumbar 4-5 level for 20 days. The
irrigation was repeated 4-5 times a day for 20 days. During the irrigation,
the animals were reanesthetized with the same combination used during
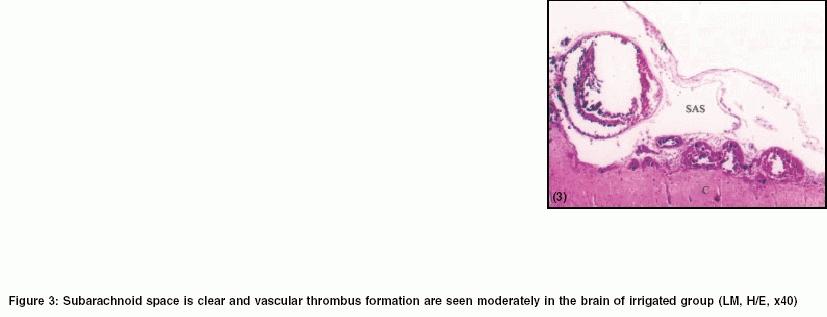
catheter insertion. Results Meningitis was fully developed in all animals within 5 days. The majority of all the infected animals had fever, epilepsy, paresia-plegia and sometimes consciousness. During therapy, clinical healing was accelerated in the irrigated animals. No animal died during the study period. Hemiplegia developed in two of the non-treated animals. Macroscopic examination of the brains showed massive swelling, abundant subarachnoidal purulent material collection, arachnoid-pia adhesions and serpinginious petechial cortical hemorrhage in Group II. Hydrocephalus was observed in 3 animals (2 from Group I, 1 from Group II [Table - 1].Histopathologically, the disease was characterized by purulent material collection in subarachnoidal and ventricular spaces together with meningovascular inflammation. An intense neutrophilic meningovascular inflammation was present in all animals in Group II. Some vessels and their branches showed marked dilatation and thrombosis. Reddish pus-like material covered, partly or totally, the surfaces of the brains. Massive infiltration of lymphocytes and neutrophilic polymorphonuclear leucocytes, a thick inflammed layer formation in the subarachnoid space, pia-cortex adhesion, sulcal stickiness and arterial thrombosis were also observed [Figure - 1]. Although meningeal and vascular inflammation persisted in non-irrigated animals [Figure - 2], these findings were mild or not observed in the irrigated animals [Figure - 3]. Findings are summarized in [Table - 2]. Histochemical parameters of the CSF (lymphocyte and mononuclear cells) also turned to normal. Discussion Meningitis is termed as a meningocerebral inflammatory response to purulent material collection in the subarachnoid and ventricular spaces. Meningitis results in cerebral ischemia, infarction, edema, cerebritis, abscess, hemorrhage, hydrocephalus and sometimes brain herniations.[2],[5] Bacterial meningitis commonly leads to death or severe neurological sequelae, including spastic or flaccid quadriparesis, mental retardation, cortical blindness, seizures and communicating hydrocephalus.[5] Acute inflammation of the meninges, vascular involvement, meningeal adhesions were the histopathological hallmarks in our animal model.Purulent CSF facilitates local bacterial growth and acts as a bacterial reservoir. The goal of therapy should be directed to an etiologic agent. Therefore, intraventricular drug administration is also advised.[1] Meningitis is often accompanied by ventriculitis and the CSF has a pus-like appearance. Early drainage of CSF and intraventricular antibiotic therapy may produce a better outcome for meningitis. In intractable meningitis cases, a ventricular drainage-irrigation system may permit an adequate perfusion of the CSF together with an antibiotic to the subarachnoid space. Continuous intraventricular irrigation in ventriculitis cases was reported in the previous studies.[6] Meningitis may cause subarachnoid hemorrhage, and cisternal drainage can result in a rapid clearance of CSF in patients with subarachnoid hemorrhage.[7] An intraventricular lavage was performed in post-traumatic ventriculitis and meningitis cases and it was repeated until the postoperative 7th day and the CSF data improved immediately.[3],[8],[15],[17] It was also reported that ventricular lavage in combination with spinal drainage might result in a good outcome in such cases.[8] After CSF clears, shunting procedure may be considered if hydrocephalus develops.[9] Significant reduction occurs in CSF formation in ventriculitis due to inflammation of the choroid plexuses. Inflammation of the arteries and veins of the choroid plexuses may also lead to a decrease in CSF production,[10] which in turn contribute to the occlusion of vessels and CSF circulation. Therefore, CSF replacement may prevent complications developing as a consequence of depleted CSF.[11],[12],[13] The possibility of cerebral infarction is also significantly higher in patients without irrigation than in those with irrigation in ventriculitis,[14] and such cases were treated with external ventricular drainage by Bayston et al.[15] It was also reported that therapeutic intraventricular lavage could be performed in ventriculitis or hemorrhagic cases.[16],[17],[18] It was claimed that irrigation therapies have been found to be effective in lysing subarachnoid clot and preventing vasospasm and infarction safely.[19] Schmidt et al[20] have shown that despite a reduction of CSF bacterial titers and leucocyte counts by CSF filtration, the extent of neuronal damage was unaltered in experimental streptococcal meningitis. Only antibiotherapy could not be completely sufficient for the meningitis. Therefore, we suggest cisternal irrigation together with spinal drainage until obtaining clear CSF. We think that irrigation and drainage not only remove foreign materials in the CSF but also prevent disturbances seen in cerebral circulation due to vasculo-occlusive factors observed in meningitis. Reduced CSF may cause subarachnoid space narrowing, arachnoid-piamater and vascular wall adhesions and arachnoid villus occlusions may result in circulation disorders both in blood and CSF circulation. Therefore, cisternal irrigation and CSF replacement procedure may prevent brain herniations by reducing the risk of hydrocephalus development and brain edema, and other complications seen in meningitis. The findings of this experimental study support and confirm the beneficial effects of the use of irrigation in the treatment of meningitis. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05026f3.jpg] [ni05026f1.jpg] [ni05026f2.jpg] [ni05026t1.jpg] [ni05026t2.jpg] |
| |||||||||

![[Table - 1]](/showimage?ni/photo/ni05026t1.jpg){kind=link}
![[Figure - 1]](/showimage?ni/photo/ni05026f1.jpg){kind=link}
![[Figure - 2]](/showimage?ni/photo/ni05026f2.jpg){kind=link}
{kind=link}
![[Table - 2]](/showimage?ni/photo/ni05026t2.jpg){kind=link}