 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
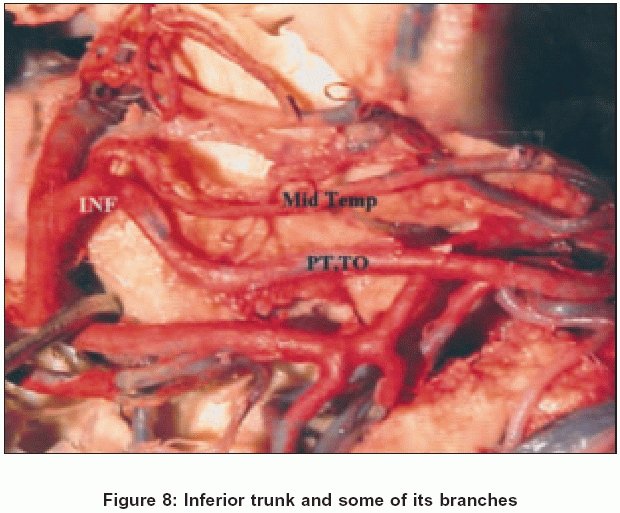
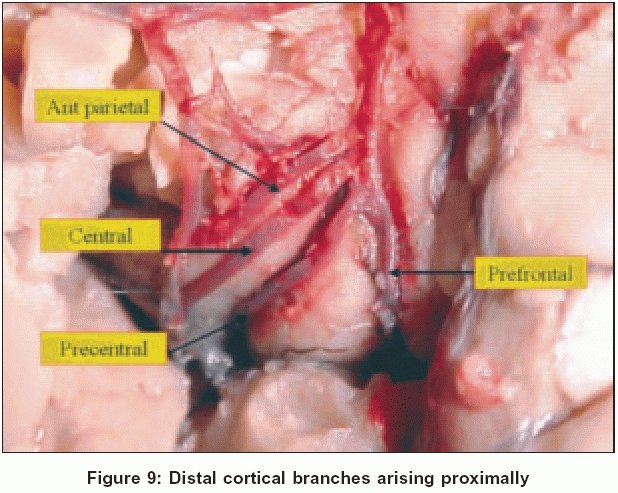
Neurology India, Vol. 53, No. 2, April-June, 2005, pp. 186-190 Original Article Microsurgical anatomy of the middle cerebral artery Pai S. Balaji, Varma R.G., Kulkarni R.N. Departments of Neurosurgery, M.S. Ramaiah Medical College, Bangalore Correspondence Address: 737, 14 th cross, Girinagar II Phase, Bangalore, balajipai65@yahoo.co.in Date of Acceptance: 09-Mar-2005 Code Number: ni05055 ABSTRACT Background: The microsurgical anatomy of the middle cerebral artery (MCA) is of particular interest to the cerebrovascular surgeon. The purpose of this study was to define the microsurgical anatomy of the MCA and its various branches in the Indian population.Methods: Ten MCAs were studied from five cadaveric brain specimens. The authors studied the outer diameter, length, branches, perforators and site of these on the main trunk (M1), the division of the main trunk, the secondary trunks and their various cortical branches using the operating microscope under 5-20x magnification. Results: The outer diameter of the MCA main trunk ranges from 2.5 to 4 mm with a mean of 3.35 mm. The superolateral branches consisted of polar temporal artery and anterior temporal artery that had a common origin and sometimes the uncal artery or the accessory uncal artery. Perforators or lenticulostriate arteries were seen in the inferomedial surface all along the length of M1. Eight bifurcations and two trifurcations were noted. Cortical branches and their origin are discussed. Conclusion: Although the microsurgical anatomy of the MCA in Indian population correlated with the findings in the western literature, some structural and statistical variations were noted. Keywords: Lenticulostriate arteries, microsurgical anatomy, middle cerebral artery, perforators Anatomical studies, both gross and microsurgical, of the middle cerebral artery (MCA) have been carried out by various authors.[1] Middle cerebral artery aneurysms form about 18.4% of all cerebral aneurysms and a thorough knowledge of the microanatomy of the MCA is essential to tackle these surgically.[2] The advent of microneurosurgical techniques resulted in the study of the microanatomy of the MCA. The purpose of this study was to define the microsurgical anatomy of the MCA and its various branches in the Indian population. MATERIALS AND METHODS We have studied ten MCAs derived from five cadaveric brain specimens. Microscopic dissection was carried out from the internal carotid artery (ICA), bifurcation through the MCA main stem (M1), bifurcation and secondary trunks (M2), and its various branches (M3 and M4). Microscopic dissection was done using the Serwell operating microscope under 5x, 10x, and 20x magnification. Particular attention was paid to the perforators arising from the M1 portion of the MCA. The division of the main trunk and the secondary trunks was studied and documented. The secondary trunks are referred to as superior, middle (if present) and inferior trunks depending on the way in which the main trunk of the MCA is divided. The MCA and its branches were painted with red watercolor and photographs taken using a digital camera to document the various situations.RESULTS The MCA originates at the bifurcation of the ICA as the larger and more direct branch. It originates lateral to the optic chiasma and courses laterally and slightly anteriorly, inferior to the anterior perforated substance (APS) to reach the medial end of the Sylvian fissure (M1). The M1 segment is the sphenoidal segment and lies posterior and parallel to the sphenoidal ridge. The artery then crosses over the limen insulae and enters the insular area where it divides into its secondary trunks - superior and inferior trunks (M2) and is referred to as the insular segment. These secondary trunks course over the insular cortex and give rise to the cortical branches. These branches turn around the operculum (M3) and then spread out over the cerebral convexity (M4). M3 is often referred to as the opercular segment and M4 as the cortical segment.Main trunk The ICA outer diameter (OD) just proximal to its bifurcation ranged from 4 to 5.5 mm. The MCA at its origin had an OD ranging from 2.5 to 4 mm with a mean of 3.35 mm. In eight cases, the MCA was larger in diameter than the anterior cerebral artery (ACA). However, it was seen to be equal in two cases. In all cases, the blood flow from the ICA was directed towards the MCA. The length of the MCA ranged widely from 12 to 28 mm with a mean of 20 mm. The branches of the main trunk (M1) can be divided into two groups of vessels. Superolateral group These branches arose from the superolateral surface of the M1 segment and consist of the uncal artery (UA), polar temporal artery (PoTA), and the anterior temporal artery (ATA). The UA was seen in all cases, but was seen to be a branch of the M1 in only four cases [Figure - 1]. It was seen to originate from the ICA in three cases and from the anterior choroidal artery in three cases. Accessory UA was also noted as a branch of M1 in four cases. In two of these situations, the UA did not originate from M1, but from the ICA and anterior choroidal artery. In all cases, the PoTA, and the ATA arose as a common trunk. It was difficult to decide whether one artery was absent leading to the hypertrophy of the other or the origin was genuinely common. The PoTA supplies the anterior temporal pole of the superior, middle and inferior temporal gyri. In two cases, the middle temporal artery (MTA), and the posterior temporal artery (PTA) arose as a common trunk from the M1 segment. In another two cases, the UA and accessory UA originated as a common trunk. Inferomedial group (lenticulostriate vessels) These arteries arise from the inferomedial surface, form vascular loops and enter the lateral portion of the APS to supply the subcortical areas of the brain [Figure - 2]. These perforators varied from 3 to 11 in number with a mean of seven in each M1. The M1 segment was divided into proximal, middle and distal portions. The perforators were found to be distributed in all the segments of M1. In two situations, perforators were noted after the MCA bifurcation - one from the superior trunk and in another case from the inferior trunk. In three situations, these vessels were seen to arise as a common origin along with the orbitofrontal artery and sometimes the prefrontal artery. When this anatomical arrangement occurs and if the orbitofrontal artery is large, one can be misled to believe that this could be the M1 bifurcation.[3] However, no lenticulostriate branches were noted from the superolateral branches of M1. Middle cerebral artery (MCA) bifurcation The bifurcation of the MCA occurs at the high point of the limen insulae. The MCA usually divides into the superior and inferior trunks [Figure - 3]. The area of the bifurcation may also be described as forming an ′omega′ pattern because of the initial divergent and then convergent courses of the secondary trunks [Figure - 4]. There were eight bifurcations and two trifurcations in our series [Figure - 5]. Among the former, there were two cases where the superior trunk divided immediately after its origin, giving a false impression of a trifurcation (pseudotrifurcation) [Figure - 6]. Both the trifurcations were seen in the same patient on opposite sides. The middle trunk divided into the angular, central, and anterior parietal (AP) branches on one side and posterior parietal and temporo-occipital on the other side. The OD of the secondary trunks was directly proportional to the number of cortical branches that arose from it. Cortical branches (M3 and M4) The anatomy and distribution of the cortical branches of the MCA have been extensively described.[1] The origins of these cortical branches can be seen on dissecting the insular segment of the MCA. However, it was necessary to follow them to the cerebral convexity to identify these branches by their area of supply. The cortical branches that were present fairly consistently were - the orbitofrontal, prefrontal, precentral, central, AP, posterior parietal, middle temporal, posterior temporal, temporo-occipital, and angular arteries. In our study, the orbitofrontal, prefrontal, precentral, central, and AP arteries owed their origins to the superior trunk in most situations [Figure - 7]. Similarly the posterior parietal, middle temporal, posterior temporal, temporo-occipital, and angular arteries took their origins from the inferior trunk [Figure - 8]. In the two MCA trifurcations that were noted, the middle trunk gave rise to the posterior parietal and temporo-occipital arteries (inferior trunk branches) in one case and AP, central, and angular arteries (superior trunk branches) in the other. The distribution of the origins of the various cortical branches is shown in [Table - 1] and [Table - 2]. Though usually the proximal branches originated proximally from the secondary trunk, this was not always the rule. [Figure - 9] shows the distal branches originating proximally. DISCUSSION The microsurgical anatomy of the MCA has interested many researchers over the years especially with the advent of microneurosurgical techniques in cerebrovascular surgery. Chater et al . (1976), Grand (1980), Gibo et al . (1981), Umansky et al . (1984), and Yasargil were the principal ones.[1]Various methods of cadaveric intravascular injections have been tried with different fixing techniques. Umansky et al . have enumerated the different injection techniques in their review article. The addition of red pigment in the intra-arterial injection makes it easy to recognize very small branches and to differentiate them from arachnoid strands. In our study however, good illumination, magnification (5-20x) and meticulous dissection were used to overcome the above deficiency. The mean length of the M1 segment in our study was 20 mm, about 5 mm longer than the others (Umansky et al ., 15.1 and 15.7 mm; Yasargil, 14-16 mm]. The M1 mean OD of 3.35 mm was nearly the same as those named by Umansky and Yasargil.[1],[3] The MCA perforators arose from its inferomedial surface in all cases. They were evenly distributed along the M1 segment. Hence, temporary clipping of the MCA during surgery cannot be considered absolutely safe, as perforators in the segment distal to the clip would be devoid of blood supply. Temporary clipping if found to be essential should be applied as distally as possible in the M1 segment. Further, exposure of the MCA should be done along the lateral border, as there are no perforators on this surface. The superolateral group in our series consisted of usually two branches - common origin of PoTA and ATA and sometimes the UA. The UA was usually a branch of the ICA or the anterior choroidal artery. The common origin of the PoTA and ATA was seen in all cases, which is not so frequent in the other studies. Perforators of the M2 segment were seen in only two cases and in these cases the M1 segment was found to be 21 and 22 mm. Yasargil reported the incidence of 10% of perforators from superior and inferior trunks.[3] In such situations, MCA bifurcation aneurysm if present would be intimately related to the perforators. Umansky et al . reported 79% of the perforators from the M1, 15.3% from secondary trunks, and 5.7% from early temporal and frontal branches.[1] Kaplan and Ford have studied the relationship of the origin of the lateral lenticulostriate arteries to the length of the M1. They noted that if the M1 length was less than 25 mm there were lenticulostriate arteries arising from or near the MCA bifurcation and even from the secondary trunks.[4] This was in contrast to our findings where no MCA was more than 28 mm (mean 20 mm). M1 bifurcation and trifurcation incidence was the same as seen by Yasargil et al . and Umansky et al . The authors opine that the exact microanatomy of this division can be ascertained only intraoperatively. The size of the secondary trunks depends on the number of cortical branches arising from it and consequently the area supplied. The STMC bypass surgery involves extracranial arterial anastamosis to one of the larger cortical branches. This has spawned renewed interest in the microanatomy of this segment of the MCA - M3 and M4. The distribution of origin of the cortical branches generally matched the report by Umansky et al . and Yasargil et al . Umansky et al ., however, reported that the AP artery generally originated from the inferior trunk, while in our study it originated from the superior trunk in 80% of the cases. Some of these cortical branches may be absent and the adjacent branches may share the blood flow. CONCLUSIONS REFERENCES
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05055f9.jpg] [ni05055f5.jpg] [ni05055f2.jpg] [ni05055f8.jpg] [ni05055f1.jpg] [ni05055f7.jpg] [ni05055t1.jpg] [ni05055f6.jpg] [ni05055t2.jpg] [ni05055f4.jpg] [ni05055f3.jpg] |
| |||||||||

![[Figure - 1]](/showimage?ni/photo/ni05055f1.jpg){kind=link}
![[Figure - 2]](/showimage?ni/photo/ni05055f2.jpg){kind=link}
![[Figure - 3]](/showimage?ni/photo/ni05055f3.jpg){kind=link}
![[Figure - 4]](/showimage?ni/photo/ni05055f4.jpg){kind=link}
![[Figure - 5]](/showimage?ni/photo/ni05055f5.jpg){kind=link}
![[Figure - 6]](/showimage?ni/photo/ni05055f6.jpg){kind=link}
![[Figure - 7]](/showimage?ni/photo/ni05055f7.jpg){kind=link}
{kind=link}
![[Table - 1]](/showimage?ni/photo/ni05055t1.jpg){kind=link}
![[Table - 2]](/showimage?ni/photo/ni05055t2.jpg){kind=link}
{kind=link}