
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 53, Num. 2, 2005, pp. 202-207
|
Neurology India, Vol. 53, No. 2, April-June, 2005, pp. 202-207
Original Article
Fever is associated with third ventricular shift after intracerebral hemorrhage: Pathophysiologic implications
Deogaonkar Anupa, Georgia MichaelDe, Bae Charles, Abou-Chebl Alex, Andrefsky John
Department of Neurology, Cleveland Clinic Foundation, Cleveland
Correspondence Address: Department of Neurology, S-91, Cleveland
Clinic Foundation, 9500, Euclid Avenue, Cleveland 44195, Ohio, degeorm@ccf.org
Date of Acceptance: 06-Feb-2005
Code Number: ni05060
Related article: ni05061
ABSTRACT
Background: Studies have shown the detrimental effect of increased
temperature on brain injury. Fever is common after intracerebral hemorrhage
(ICH). The term "central fever" ? is often used when no cause is identified.
Aim: The aim of the study was to determine the correlation of fever with third ventricular shift in 61 patients with ICH and hypothesize about the mechanism of fever.
Setting: Neurointensive Care Unit
Design: Prospective observational study.
Materials and Methods: From August 1999 to April 2000, data from 61 patients with ICH were prospectively collected including maximum temperature (Tmax) and fever (T >37.5° C) at 24, 48, 72 and 96 hours, ICH volume, and third ventricular shift. Outcome measures included discharge mortality, 3-month National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), and Barthel Index (BI).
Statistical Analysis: Spearman correlation coefficient, Mann-Whitney test, and logistic regression were used to assess relationships.
Results: Fifty-six per cent of patients had fever in the first 24 hours and 53% for at least two consecutive days. There was a correlation between ICH volume and Tmax at 24 hours ( P =0.04) and 72 hours ( P =0.03) and fever at 24 hours ( P =0.039) and 72 hours ( P =0.036). Tmax at 72 hours correlated with third ventricular shift ( P =0.01). Those with shift were more likely to have fever within the first 72 hours ( P =0.049) and worse outcome. Fever at 72 hours was associated with a higher discharge mortality ( P =0.046) and trend of a worse 3-month NIHSS score ( P =0.06).
Conclusion: Fever is common after ICH and correlates with ICH volume and third ventricular shift suggesting a role of hypothalamic compression in "central fever." There was a trend towards a worse outcome with fever.
Keywords: Fever, intracerebral hemorrhage, hypothalamus
There is a growing body of literature demonstrating the detrimental effects of fever, whatever the cause, after brain injury. Animal models of global and focal cerebral ischemia, have shown that even mild hyperthermia exacerbates ischemic neuronal injury.[1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11] Fever is common after intracerebral hemorrhage.[12],[13] Possible causes include infections of the urinary and respiratory tract, thrombophlebitis, and drug reactions. Often the term "central fever" is used when no obvious cause can be identified. "Central fever" has most often been attributed to cytokine-related elevation of the hypothalamic set point. Mechanical compression of the hypothalamus has been demonstrated in animal models to cause fever.[14] We hypothesized that patients with third ventricular shift after ICH would be more likely to become febrile due to hypothalamic compression than patients without third ventricular shift. We analyzed 61 patients with ICH for incidence of fever and correlation with third ventricular shift.
MATERIALS AND METHODS After Institutional Review Board approval at The Cleveland Clinic Foundation, we prospectively collected data on 61 patients with spontaneous ICH, with or without intraventricular hemorrhage (between August 1999 to April 2000) consecutively admitted to the Neurological Intensive Care Unit. Exclusion criteria included subarachnoid hemorrhage (SAH), hemorrhagic transformation, subdural hematoma, epidural hematoma, hospital admission >24 hours, prior ischemic stroke. Data collected included age, gender, race, vascular risk factors, Glasgow Coma Scale (GCS) score and National Institute of Health Stroke Scale (NIHSS) score on admission. Hemorrhage location and volume were recorded from the admission brain Computerized Tomography (CT) scan (volume was calculated using the ABC/2 method).[15],[16] The presence of third ventricular shift was determined from admission brain CT scan by a neuroradiologist blinded to the patients′ clinical status and temperature. The amount of shift was classified as mild (1-5 mm), moderate (5-10 mm), or severe (>10 mm). Hourly temperatures and maximal temperatures (Tmax) at 24, 48, 72 and 96 hours were recorded. Fever was defined as a body temperature greater than 37.5°C. Patient outcome measures included NIHSS score, modified Rankin Scale (mRS) score, and Barthel Index (BI) at 96 hours, at 1 week, at discharge and at 3 months.
Statistical analysis: Spearman Correlation Coefficient, Mann Whitney test and logistic regression analysis were used to assess relationships. Odds ratios (OR) and 95% confidence intervals (CI) are reported for each comparison. No adjustment was made for multiple comparisons over time.
RESULTS
Out of 61 patients in the study, 25 (41%) were males and 36 (59%) were females. Demographic data for the 61 patients are reported in [Table - 1]. The mean age was 65±16 years (range 30-92). The mean admission GCS score was 8.8±4.8 and the mean NIHSS score was 20.05±11.5. The most common hemorrhage location was lobar (63%) followed by deep basal ganglia (27%) and infratentorial (10%). The mean ICH volume was 48.9±52.4 ml. Fifty-six percent of patients had fever in the first 24 hours, 53% had fever for at least two consecutive days. The mean Tmax overall was 38.0±0.9o C. The mean Tmax in the first 72 hours was 38.5±0.9o C. Thirty-two of 58 patients (55.1%:
data missing in 3 patients) had third ventricular shift greater than 1
mm [Figure - 1]. Fifteen of these 32 patients (47%) had mild shift, 9 (28%) had moderate shift and 8 (25%) had severe shift of the third ventricle. Overall, the mean third ventricular shift was 3.6±4.5 mm. There was a correlation between the presence of third ventricular shift and Tmax at 72 hours ( P =0.01, SSC=0.37) and between third ventricular shift and presence of fever within 72 hours ( P =0.049, SSC=0.37). Fifty-nine per cent vs. 44% patients had fever during the first 24 hours, 64% vs. 48% patients had fever during 24-48 hours and 86% vs. 46% had fever during 48-72 hours in patients with shift as compared to patients without shift ( P =0.09). [Table - 2] shows incidence of infection, intubation and presence of deep vein thrombosis (DVT) in all patients. Multivariate analysis showed no confounding effects of infection, intubation or thrombophlebitis.
There was a correlation between ICH volume and Tmax at 24 hours ( P =0.04, SCC=0.26) and at 72 hours ( P =0.03, SCC=0.32). There was also a correlation between ICH volume and the presence of fever at 24 hours ( P =0.039, SCC= 0.26) and at 72 hours ( P =0.036, SCC=0.32) [Table - 3]. Models predicting hospital mortality using baseline NIHSS, GCS, ICH volume and other covariables are described in [Table - 4]. NIHSS and GCS were not shown to differ on the prediction of hospital mortality. Other factors were not important predictors of mortality.
[Table - 5] shows correlation between baseline scales and functional outcome at 3 months for all patients. Baseline NIHSS and ICH volume correlated with 3-month outcomes than GCS and ICH volume. Fever at 72 hours was associated with a higher mortality rate ( P =0.046) and a trend of a worse NIHSS score at 3 months ( P =0.06). No worse outcome was observed when measured by Barthel Index or mRS.
Univariate analysis of shift and continuous outcome at 3 months showed that patients with any shift have poor outcome ( P =0.015 for NIHSS, P =0.014 for Barthel′s Index, P =0.015 for mRS) and are 3.3 times more likely to die at discharge vs. those with no shift ( P =0.027). Even after adjusting for fever in multivariate analysis, in all patients, any shift was associated with poorer outcome at 3 months than no shift ( P =0.015 for NIHSS, P =0.014 for Barthel′s Index, P =0.015 for mRS).
DISCUSSION
Our study demonstrates a correlation of fever with ICH volume and third ventricular shift. There was a correlation between ICH volume and Tmax at 24 hours and at 72 hours. There was also a correlation between ICH volume and the presence of fever at 24 hours. In our study, fever at 72 hours after ICH was associated with a higher mortality rate and a trend towards a worse neurological outcome at 3 months.
It has long been recognized that fever is common following brain injury and particularly in patients with ICH. Aring and Merrit, in 1935, were the first to report that fever was more common in patients with hemorrhagic stroke compared with ischemic stroke.[17] This has been further confirmed by more recent studies. Kilpatrick and coworkers reported that among patients admitted to a neurological intensive care unit, those with SAH and ICH had the highest incidence of fever.[13] Estratopoulos
and coworkers reported fever in 85% of patients with primary ICH
within the first 48 hours.[18] Schwarz
and coworkers reported fever in 91% of patients in the first 72
hours.[12] In our study,
over half of the patients (56%) had fever within the first 24
hours of admission to the neurological intensive care unit.
Common causes of fever after ICH include infections of the urinary and
respiratory tract, thrombophlebitis, and drug reactions. Often the term "central fever" is used in patients when no cause can be identified. "Central fever" has
most often been attributed to cytokine-related elevation of the hypothalamic
set point.[14] Experimental
models suggest that elevated prostaglandin levels (PG-E2) and thromboxane
B2 may also play a role in "central fever".[19] Direct hypothalamic damage can also cause fever. Elevated body temperature in rats has been induced with anterior and preoptic ischemia[20] and medial hypothalamic ischemia.[21] Fever has been induced by direct injury of the hypothalamus from acute mechanical puncture[22] or electrical shock.[23] Clar and coworkers, in a rat model, showed reversible disturbances in temperature regulation from direct hypothalamic compression.[24] In
our study, correlation of fever with hemorrhage volume and third ventricular
shift suggests a possible role of hypothalamic compression as a cause
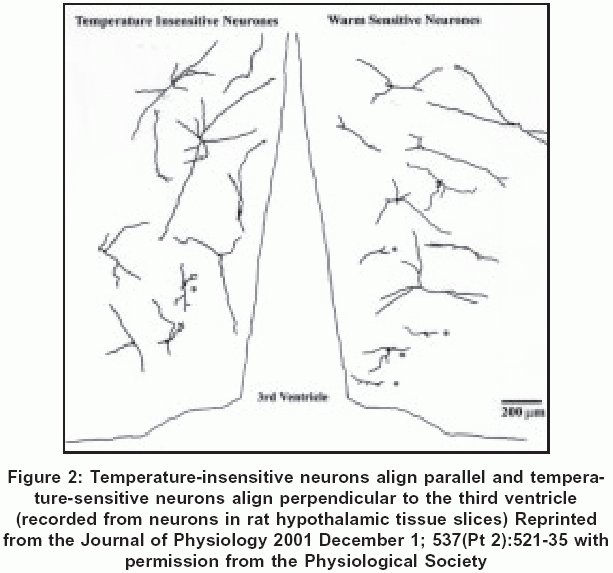
of "central fever." Anatomically, temperature-sensitive neurons in the
hypothalamus are oriented perpendicular to the third ventricle such that
dendrites project both laterally, to receive information from ascending
fibers of the median forebrain bundle, and medially, to receive information
from periventricular fibers and cerebrospinal fluid.[25] This morphology of temperature-sensitive and temperature-insensitive neurons around the third ventricle is shown in [Figure
- 2]. A large hemorrhage volume that results in the shift of the third ventricle may cause these hypothalamic dendrites to buckle and thereby disrupt temperature homeostasis.
Fever is associated with a worse outcome after brain injury.[26],[27],[28] A recent meta-analysis showed that in patients with ischemic stroke, fever is associated with a marked increase in morbidity and mortality.[29],[30],[31],[32],[33],[34] Few studies have examined the relationship of fever and outcome in patients with intracerebral hemorrhage. Schwarz and coworkers found that fever was independently associated with a worse outcome.[12] A recently reported study by Szczudlik et al[35] demonstrated that increased body temperature is not an independent predictor of 30-day mortality after ICH. However, the authors concluded that patients with hyperthermia on the first day of hospitalization have greater 30-day mortality and worse functional status 30 days after stroke, but increased body temperature is not an independent predictor of 30-day mortality after ICH. In our study, fever at 72 hours after ICH was associated with a higher mortality rate and a trend towards a worse neurological outcome at 3 months.
Limitations of this study include the small patient population and inconsistent temperature monitoring. A larger prospective study with continuous temperature monitoring is required to confirm our findings. Although it has been previously shown by Arboix et al[36] that the site of bleeding determines the clinical spectrum and in-hospital mortality in spontaneous ICH, our results were not analyzed to study the outcome according to the site of bleeding.
In summary, our results show that the incidence of fever after ICH is
high with most patients having fever in the first 24 hours after admission.
Correlation of fever with hemorrhage volume and third ventricular shift
suggests a possible role of hypothalamic compression in "central fever" after
ICH. There was a trend towards a worse outcome with fever in our patients.
REFERENCES
| 1. | Baena RC, Busto R, Dietrich WD, Globus MY, Ginsberg MD. Hyperthermia delayed by 24 hours aggravates neuronal damage in rat hippocampus following global ischemia. Neurology 1997;48:768-73. Back to cited text no. 1 [PUBMED] |
| 2. | Busto R, Dietrich WD, Globus MY, Valdes I, Scheinberg P, Ginsberg M. Small differences in intra-ischemic brain temperature critically determine the extent of ischemic neuronal injury. J Cereb Blood Flow Metab 1987;7:729-38. Back to cited text no. 2 |
| 3. | Dietrich WD, Alonso O, Halley M, Busto R. Delayed posttraumatic brain hyperthermia worsens outcome after fluid percussion brain injury: A light and electron microscopic study in rats. Neurosurgery 1996;38:533-41. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Coimbra C, Boris-Moller F, Drake M, Wieloch T. Diminished neuronal damage in the rat brain by late treatment with the antipyretic drug dipyrone or cooling following cerebral ischemia. Acta Neuropathol (Berl) 1996;92:447-53. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Coimbra C, Drake M, Boris-Moller F, Wieloch T. Long-lasting neuroprotective effect of postischemic hypothermia and treatment with an anti-inflammatory/antipyretic drug. Evidence for chronic encephalopathic processes following ischemia. Stroke 1996;27:1578-85. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Dietrich WD, Busto R, Valdes I, Loor Y. Effects of normothermic versus mild hyperthermic forebrain ischemia in rats. Stroke 1990;21:1318-25. Back to cited text no. 6 [PUBMED] |
| 7. | Ginsberg MD, Busto R. Combating hyperthermia in acute stroke: A significant clinical concern. Stroke 1998;29:529-34. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Kim Y, Busto R, Dietrich WD, Kraydieh S, Ginsberg MD. Delayed postischemic hyperthermia in awake rats worsens the histopathological outcome of transient focal cerebral ischemia. Stroke 1996;27:2274-80. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Meden P, Overgaard K, Pedersen H, Boysen G. The influence of body temperature on infarct volume and thrombolytic therapy in a rat embolic stroke model. Brain Res 1994;647:131-8. Back to cited text no. 9 [PUBMED] |
| 10. | Memezawa H, Zhao Q, Smith ML, Siesjo BK. Hyperthermia nullifies the ameliorating effect of dizoclipine maleate (MK-801) in focal cerebral ischemia. Brain Res 1995;670:48-52. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Minamisawa H, Smith ML, Siesjo BK. The effect of mild hyperthermia and hypothermia on brain damage following 5, 10, and 15 minutes of forebrain ischemia. Ann Neurol 1990;28:26-33. Back to cited text no. 11 [PUBMED] |
| 12. | Schwarz S, Hafner K, Aschoff A, Schwab S. Incidence and prognostic significance of fever following intracerebral hemorrhage. Neurology 2000;54:354-61. Back to cited text no. 12 [PUBMED] [FULLTEXT] |
| 13. | Kilpatrick M, Lowry D, Firlik A, Yonas H, Marion D. Hyperthermia in the neurosurgical intensive care unit. Neurosurgery 2000;47;4:850-5. Back to cited text no. 13 |
| 14. | Dinarello C, Cannon J, Wolff S. New concepts on the pathogenesis of fever. Rev Infect Dis 1988;101:168-89. Back to cited text no. 14 |
| 15. | Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volume of intracerebral hemorrhage: A powerful and easy-to-use predictor of 30-day mortality. Stroke 1993;24:987-93. Back to cited text no. 15 [PUBMED] |
| 16. | Broderick JP, Brott T, Grotta J. Intracerebral hemorrhage volume measurement. Stroke 1994;25;5:1081. Back to cited text no. 16 |
| 17. | Aring C, Merritt H. Differential diagnosis between cerebral hemorrhage and cerebral thrombosis; a clinical and pathological study of 245 cases. Arch Intern Med 1935;56:435-56. Back to cited text no. 17 |
| 18. | Estratopoulos A, Voyaki S, Leuow M. Fever from intracerebral hemorrhage. therapeutic effect of Naproxen. presented in 56th International Conference of Stroke and 2nd Conference of the Mediterranean Stroke Society 2001. Istanbul, Turkey. (Abstract) Back to cited text no. 18 |
| 19. | Dewitt D, Kong D, Lyeth B, Jenkins L, Hayes R, Wooten E, et al . Experimental traumatic brain injury elevates brain prostaglandin E2 and thromboxane B2 levels in rats. J Neurotrauma 1988;5:303-13. Back to cited text no. 19 |
| 20. | Zhao Q, Memezawa H, Smith M, Siesjo B. Hyperthermia complicates middle cerebral artery occlusion induced by an intraluminal filament. Brain Res 1994;649:253-9. Back to cited text no. 20 |
| 21. | He Z, Yamawaki T, Yang S, Day AL, Simpkins JW, Naritomi H. Experimental model of small deep infarcts involving the hypothalamus in rats: Changes in body temperature and postural reflex. Stroke 1999;30:2743-51. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Ackerman D, Rudy T. Thermoregulatory characteristics of neurogenic hyperthermia in the rat. J Physiol 1980;307:59-70. Back to cited text no. 22 |
| 23. | Nathan MA, Reis D. Fulminating arterial hypertension with pulmonary edema from release of adrenomedullary catecholamines after lesions of the anterior hypothalamus in the rat. Circ Res 1975;37:226-35. Back to cited text no. 23 |
| 24. | Clar HE, Disturbances of the hypothalamic thermoregulation. Acta Neurochir (Wien) 1985;75;106-12. Back to cited text no. 24 |
| 25. | Griffin JD, Saper CB, Boulant JA, Synaptic and morphological characteristics of temperature-sensitive and -insensitive rat hypothalamic neurones. J Physiol 2001;537:521-35. Back to cited text no. 25 |
| 26. | Sazbon L, Groswasser Z. Outcome in 134 patients with prolonged posttraumatic unawareness. Part 1: Parameters determining late recovery of consciousness. J Neurosurg 1990;72:75-80. Back to cited text no. 26 [PUBMED] |
| 27. | Stover SL, Zeiger HE Jr. Head injury in children and teenagers; functional recovery correlated with the duration of coma. Arch Phys Med Rehabil 1976;57:201-5. Back to cited text no. 27 [PUBMED] |
| 28. | Auer LM, Gell G, Richling B, Oberbauer R, Clarici G, Heppner F. Predicting lethal outcome after severe head injury- a computer-assisted analysis of neurological symptoms and laboratory values. Acta Neurochir (Wien) 1980;52:225-38. Back to cited text no. 28 [PUBMED] |
| 29. | Reith J, Jorgensen HS, Pedersen PM, Nakayama H, Raaschou HO, Jeppesen LL, et al . Body temperature in acute stroke: relation to stroke severity, infarct size, mortality, and outcome. Lancet 1996;347:422-5. Back to cited text no. 29 |
| 30. | Hajat C, Hajat S, Sharma P, Effects of poststroke pyrexia on stroke outcome: A meta-analysis of studies in patients. Stroke 2000;31:410-4. Back to cited text no. 30 |
| 31. | Azzimondi G, Bassein L, Nonino F, Fiorani L, Vignatelli L, Re G, et al . Fever in acute stroke worsens prognosis- A prospective study. Stroke 1995;26:2040-3. Back to cited text no. 31 |
| 32. | Castillo J, Davalos A, Marrugat J, Noya M. Timing for fever-related brain damage in acute ischemic stroke. Stroke 1998;29:2455-60. Back to cited text no. 32 [PUBMED] [FULLTEXT] |
| 33. | Hindfelt B. The prognostic significance of subfebrility and fever in ischemic cerebral infarction. Acta Neurol Scand 1976;53:72-9. Back to cited text no. 33 [PUBMED] |
| 34. | Greisman L, Mackowiak P. Fever: beneficial and detrimental effects of antipyretics. Curr Opin Infect Dis 2002;15:241-5. Back to cited text no. 34 |
| 35. | Szczudlik A, Turaj W, Slowik A, Strojny J. Hyperthermia is not an independent predictor of greater mortality in patients with primary intracerebral hemorrhage. Med Sci Monit 2002;8:702-7. Back to cited text no. 35 [PUBMED] [FULLTEXT] |
| 36. | Arboix A, Comes E, Garcia-Eroles L, Massons J, Oliveres M, Balcells M, et al . Site of bleeding and early outcome in primary intracerebral hemorrhage; Acta Neurol Scand 2002;105:282-8. Back to cited text no. 36 |
Copyright 2005 - Neurology India
The following images related to this document are available:
Photo images
[ni05060t1.jpg]
[ni05060f2.jpg]
[ni05060t3.jpg]
[ni05060t5.jpg]
[ni05060f1.jpg]
[ni05060t2.jpg]
[ni05060t4.jpg]
|

![[Figure - 1]](/showimage?ni/photo/ni05060f1.jpg){kind=link}
{kind=link}