 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
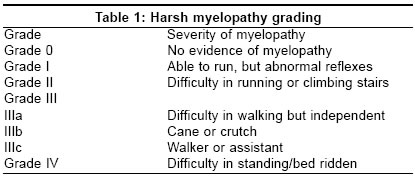
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 283-285 Original Article Multisegmental cervical ossification of the posterior longitudinal ligament: Anterior vs posterior approach Jain SubodhK, Salunke PravinS, Vyas KH, Behari SanjayS, Banerji Deepu, Jain VijendraK Department of Neurosurgery, Sanjay Gandhi Post Graduate Institute Of Medical Sciences, Raebareli Road, Lucknow, Uttar Pradesh Date of Acceptance: 05-Jun-2005 Code Number: ni05096 Related article: ni05097 Abstract Aims : To determine the surgical approach in patients with multisegmental (four or more segments) OPLL of the cervical spine.Methods and Materials : Data of 27 patients who had undergone either an anterior (corpectomy with excision of OPLL and interbody fusion=14 patients) or posterior approach (laminectomy=12, laminoplasty=1 patient) for the multisegmental cervical OPLL was analyzed retrospectively. The patients in each group were statistically similar in respect to preoperative factors such as age, duration of symptoms, preoperative modified Japanese orthopedic association score, OPLL thickness, effective canal diameter, and antero-posterior cord compression ratio. The clinical outcome was assessed by the Harsh grading system and recovery rate was assessed by Hirabayashi method. Results : There was no statistical difference in the outcome, and recovery rate. Nine patients developed complications after anterior approach in contrast to one after posterior approach. Conclusions : In patients with multisegmental cervical OPLL, there was no significant difference in the short-term recovery rate and outcome between two groups. The immediate postoperative complications were less in patients who had undergone posterior approach. From our analysis, it appears that the posterior approach is probably the preferred method of treatment in a multisegmental OPLL in absence of preoperative kyphosis. Keywords: cervical spine; laminoplasty; ossification of the posterior longitudinal ligament; spinal instrumentation. Several previous studies have analyzed the results of anterior or posterior surgical approach in patients with ossification of the posterior longitudinal ligament (OPLL) of the cervical spine. [1],[2],[3],[4],[5] In this study, we compare the results of anterior and posterior surgical approach in an identical cohort of patients having multisegmental cervical OPLL. Materials and methods During the period between January 1996 and January 2004, 55 patients with cervical OPLL were operated. These patients were analyzed retrospectively. Twenty-seven patients had multisegmental OPLL (four or more segments). Out of 27 patients, 14 underwent anterior approach (corpectomy with excision of OPLL and interbody fusion using iliac crest bone graft). Three-level corpectomy was done in 13 patients and four-level corpectomy was done in one patient. Metal instrumentation was not done in any patient. The remaining 13 patients underwent posterior approach. C2-7 laminectomy was done in 12 patients and open door laminoplasty (C2-7) was done in one patient. In seven cases of laminectomy and one of laminoplasty pneumatic drill was used. For the remaining five patients laminectomy was done using roungers and micropunches. There were four patients who had cervical kyphosis or straight spine and all of them underwent an anterior approach. For the remaining 23 patients the criteria for any particular approach were not outlined. The severity of myelopathy was assessed using Harsh grading scale in all the patients [Table - 1].[6] Considering the added advantage of modified Japanese orthopedic association score (mJOAS) over Harsh grade in assessing the motor and sensory deficits along with disability and sphincteric dysfunction, all patients were also assessed using mJOAS.[7],[8] The curvature of spine, maximum OPLL thickness and the effective canal diameters were measured on plain X-ray. Type of OPLL was classified according to Hirabayashi classification.[9] (Segmental: located behind the vertebral body; continuous: extends from body to body; mixed: both segmental and continuous components; others: confined to disc space.) Antero-posterior cord compression ratio (APCR) was measured as the percentage ratio of smallest sagittal to maximum transverse diameter of the cord at the level of compression on T1 weighted, axial MRI [Figure - 1].[10]
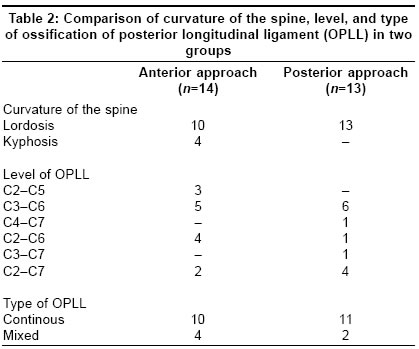
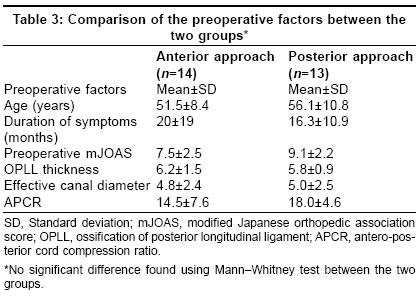
Post operative mJOAS - Preoperative mJOAS X 100. Mean follow-up period was 13 months, which was similar for both the groups, with maximum follow up of 36 months. At follow up, the neurological improvement or deterioration was assessed by two parameters, i.e., outcome and recovery rate. The outcome could be good (Harsh grades I, II), fair (Harsh IIIa, IIIb), or poor (Harsh IIIc, IV). The recovery rate was used to quantify the extent of neurological improvement or deterioration. The ′Recovery rate′was calculated in percentage by the method described by Hirabayashi,[11] i.e., Statistical analysis Results Twenty-four patients were males and three were females. Age ranged from 30 to 74 years and the mean age was 53.74 (±9.8) years. The mean duration of symptoms at presentation was 18.2 (range 2-60) months. Spasticity was present in 26 (96%) patients, and motor weakness in 19 (70.4%). Ten (37%) patients had sensory dysfunction and 10 patients (37%) had sphincteric dysfunction. Six (22%) patients had radicular pain or neck pain. Three patients had history of trauma leading to deterioration. There was no difference in the curvature of spine, level and type of OPLL in the two groups [Table - 2]. Four patients had a fixed kyphotic deformity or loss of normal lordosis (straight spine). The factors like age of the patient, duration of symptoms, preoperative mJOAS, OPLL thickness, effective canal diameter, and APCR were similar in the two groups and there was no significant statistical difference ( P value>0.05 for all factors compared) [Table - 3]. The surgical outcome of patients with multisegmental cervical OPLL who had undergone anterior and posterior approach. Good outcome was observed in 71 and 61% of the patients who had undergone anterior and posterior approach, respectively. The mean recovery rate was 63.27 (±20.21) and 58.85 (±15.38) in patients with anterior and posterior approach, respectively. There was no statistical difference (using Mann-Whitney test) in number of patients with good outcome ( P =0.09), and recovery rate ( P =1.3) between the two groups. The postoperative complications in patients who had undergone a posterior approach were less frequent as compared to those with anterior approach. In the posterior surgery group, one patient worsened in power in all limbs following laminectomy but progressively improved to the preoperative status. The cause for this deterioration was not clear but was probably due to nonusage of drill. Nine patients had complications following anterior approach. Two of them had deterioration in power in all limbs, and were given methylprednisolone following which one improved to the preoperative grade and the other patient did not show any improvement. The same patient required postoperative ventilatory support for 3 days after which he could be weaned off. The cause of deterioration was probably cord handling during OPLL excision. Three patients had CSF leak from the anterior wound and required lumbar drainage. One patient had graft extrusion for which he was re-explored. The graft, which was slightly longer was refashioned and repositioned. One patient each had respiratory distress and dysphagia following surgery. There was no significant difference in the outcome, and recovery rate between the two groups. There was no mortality in either group. Discussion The advantage of anterior surgical approach in cases with multisegmental OPLL includes effective decompression of the OPLL and the possibility of prevention of progression of the OPLL.[5] However, the anterior approach is relatively more difficult and carries potential risks of graft extrusion, CSF leak, excessive venous bleeding, and dysphagia.[12] The advantages of posterior decompression is that the operation is relatively straightforward.[13] However, the possibility of progression of OPLL, postlaminectomy membrane formation, kyphotic deformity, and instability of the cervical spine remains.[3],[14],[15] For multilevel cervical spodylotic myelopathy, laminoplasty may be the preferred method of treatment in absence of preoperative kyphosis.[16] In our study, the results of anterior and posterior approach in patients with multisegmental cervical OPLL were compared. There was no significant difference in the outcome, and short-term recovery rate between the two groups. Considering the higher rate of complications with the anterior surgery group, it appears that the posterior approach could be preferable for patients with multisegmental cervical OPLL with cervical lordosis. Hirabayashi et al., analyzed the results of laminectomy in patients with OPLL and reported that the most coμn cause of deterioration was the progression of the OPLL.[11] However the follow-up period in our study is relatively short and the progression of OPLL and kyphotic deformity could not be evaluated. As laminectomy carries certain known disadvantages like kyphotic deformity, progression of OPLL, postlaminectomy membrane formation and instability of the cervical spine, it has now been commonly replaced by laminoplasty for multisegmental cervical OPLL.[5],[15] The rate of progression of the OPLL and kyphotic deformity after laminoplasty is believed to be lower than that after laminectomy.[5],[13],[15] References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05096t3.jpg] [ni05096t1.jpg] [ni05096t2.jpg] [ni05096f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}