 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 291-294 Original Article A prospective study of reversible dementias: Frequency, causes, clinical profile and results of treatment Srikanth S, Nagaraja AV1 Dementia Programme, Department of Neurology, Singapore
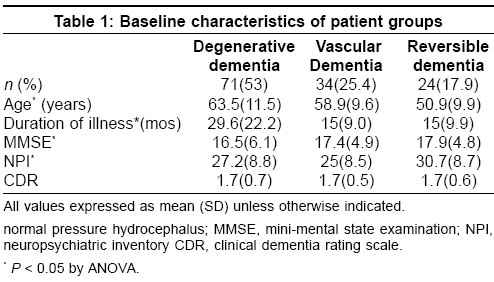
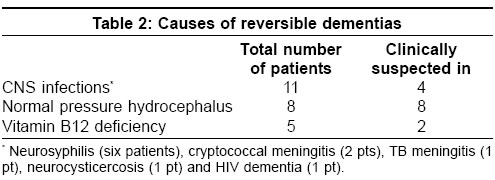
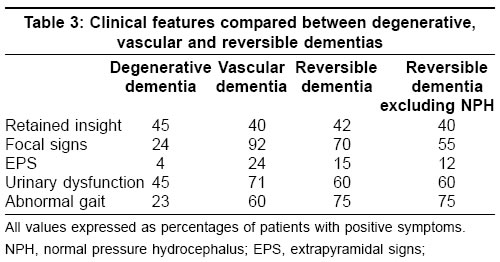
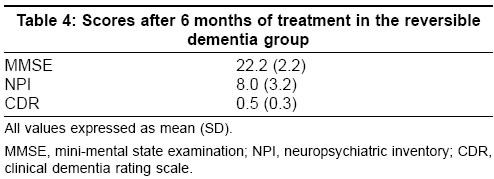
General Hospital 1 Date of Acceptance: 23-Jul-2005 Code Number: ni05100 Related article: ni05101, ni05102 Abstract Background: Dementia due to potentially reversible etiologies is an important group of dementias to be identified not only because of the number of such Patients encountered but also due to the potential for substantial improvement with treatment.Aims : To prospectively investigate the frequency and causes of dementias with potentially reversible etiologies; to examine the clinical features of this subgroup with a view to identifying a signature profile and to determine if this potential reversibility translates into actual reversibility with appropriate treatment. Setting and design : A prospective longitudinal study of patients with dementia presenting to the outpatient services of a tertiary referral hospital. Methods : All Patients above 40 years referred for evaluation of cognitive complaints were serially enrolled and underwent clinical examination, various laboratory tests and neuroimaging. Patients were followed-up for one year. Statistical analysis : One way analysis of variance for continuous variables followed by post hoc comparisons using Scheffe's procedure. Results: A total of 129 patients met Diagnostic and Statistical Manual of Mental Disorders edition 4 (DSM IV) criteria for dementia and qualified for inclusion into the study. Twenty-four patients (18%), all with moderately severe cognitive [mean mini mental state examination (MMSE) score ± SD = 17.9 ± 4.8] and neuropsychiatric [mean neuropsychiatric inventory (NPI) score ± SD = 30.7 ± 8.7] dysfunction were diagnosed to have reversible causes - neuroinfections in 11 patients, normal pressure hydrocephalus in 8 patients and vitamin B12 deficiency in 5 patients. The majority of these patients had gait and urinary dysfunction reminiscent of subcortical dementias. These reversible causes were clinically suspected in only 58% of patients. In 20/24 patients in whom follow up was possible mean MMSE score had improved to 22.2 and mean NPI score had improved to 8.0, following 6 months of treatment. Conclusions : Reversible causes, especially neuroinfections and vitamin B12 deficiency accounted for 18% all dementias in this study. The majority of these conditions was not clinically suspected though resulting in moderate to severe cognitive and psychiatric dysfunction. Most of these patients had a subcortical pattern of dementia and showed substantial improvement with treatment. Keywords: Dementia, reversible causes, neuroinfections, normal pressure hydrocephalus, vitamin B12 deficiency. Introduction Dementia is one of the most disabling disorders afflicting the elderly with staggering emotional and economic impact. It has achieved silent epidemic proportions not only in the West but in countries such as India too. The reported frequency of dementia in the community dwelling adults older than 65 years is 3 -11%[1] and increases as the population ages further,. The prevalence of dementia in India has been shown to vary from 0.84% to 3.5 %[2],[3],[4],[5],[6] in various studies. The reported frequency of dementia due to potentially reversible causes varies from 0 to 23%.[7],[8],[9] Coμnest among these causes are alcohol and medication related dementia, depression induced cognitive impairment, surgical brain lesions such as normal pressure hydrocephalus [NPH], tumors and chronic subdural hematomas, metabolic disorders such as hypothyroidism, hypoparathyroidism, vitamin B12 deficiency and central nervous system (CNS) infections such as neurosyphilis and HIV.[10] The availability of specific treatment modalities for almost all dementia subtypes makes comprehensive evaluation imperative so that potentially reversible factors contributing to the dementia syndrome can be identified and treated. However, the cost of investigating for a few causes that might be reversible has to be balanced against the benefit that would accrue to the patient in whom such a cause is identified and treated. This question is all the more important in a country like India, where on one hand the proportion of patients with dementia attributable to reversible etiologies is suspected to be higher than in the West while on the other hand the resources available to diagnose them are limited. Given these constraints careful selection of patients with dementia for work up for reversible causes assumes great importance. There has been no study from India till date that has specifically dealt with these questions. We therefore studied prospectively, patients with cognitive complaints presenting to the neurology services of our hospital with the following aims - to investigate the frequency of dementias with potentially reversible etiologies; to examine the clinical features of this subgroup with a view to identifying a signature profile and to determine if this potential reversibility translates into actual reversibility with appropriate treatment. Patients and methods This was a prospective study and consecutive patients above 40 years of age referred to the neurology services of our hospital for evaluation of cognitive complaints during a period of one year (September 2001 to October 2002) were investigated. All patients underwent neurologic, cognitive and psychiatric evaluation according to a standard protocol. After initial clinical evaluation all patients underwent standard laboratory work [including but not limited to] - complete blood counts with peripheral smear and ESR, serum chemistry for glucose, liver, renal, and thyroid function tests and serum electrolytes including calcium. Neuroimaging (computed tomography or magnetic resonance imaging) was performed in all patients. Supplementary tests like cerebrospinal fluid (CSF) examination, serum B12 assay, serological tests for syphilis, and HIV, electroencephalography and neuropsychological evaluation were performed as deemed necessary. All patients and their principal caregivers were interviewed to obtain scores on the following scales - mini-mental state examination (MMSE),[11] neuropsychiatric inventory (NPI)[12] and clinical dementia rating scale (CDR).[13] The diagnosis of dementia was by DSM IV criteria.[14] Standard published criteria were used for the diagnosis of Alzheimer′s disease (AD),[15] vascular dementia (VaD),[16] and frontotemporal dementia (FTD).[17] All other diagnoses were classified according to the International statistical classification of diseases and related health problems, tenth revision (ICD-10).[18]Patients with alcoholic dementia (3 patients), depressive pseudodementia (8 patients), intracranial tumors (3 patients), and chronic subdural hematomas (11 patients) were excluded from the present study as they were referred to the psychiatry and neurosurgery departments for further management and follow-up. Statistical analyses were performed using SPSS Version 10.0. Differences in group means of patient age, duration of symptoms and MMSE, NPI, CDR scores were analyzed for significance by one way analysis of variance [anova] followed by post hoc pairwise comparisons using the Scheffe′s procedure. For all analyses the significance level was set at P <0.05. While comparing clinical features between the different groups AD and FTD patients were merged into one group [degenerative dementia group] while the reversible dementia group was split into two - the whole group and the reversible group with NPH patients excluded. This we felt would give a truer clinical picture of dementia due to other reversible etiologies free of contamination by patients with NPH whose clinical features are already well characterized. Results One hundred and twenty nine consecutive patients with dementia met study criteria and completed the diagnostic evaluation during the study period. [Table - 1] shows the baseline characteristics of patients in the various groups. Patients in the reversible dementia group differed significantly from the other groups on age, duration of symptoms, MMSE and NPI scores. Mean dementia severity as assessed on the CDR scale did not however vary significantly between the groups. Of the 24 patients with reversible causes for dementia, 11 had neuroinfections, eight patients had normal pressure hydrocephalus (NPH) and five had vitamin B12 deficiency [Table - 2]. The largest of the subgroups within the reversible dementia cohort was the one with CNS infections. Of these eleven patients with CNS infections, 6 had neurosyphilis (one with concomitant HIV), 2 had cryptococcal meningitis (one with concomitant HIV) and one patient each had tuberculous meningitis, HIV associated dementia and neurocysticercosis. A reversible cause for dementia was clinically suspected in only 14 of these 24 patients. NPH was clinically suspected in all eight patients. However in the remaining sixteen patients, CNS infection was suspected in only 4/11 and vitamin B12 deficiency in only 2/5 patients. With regard to the clinical features of patients with reversible dementias we found that these patients were significantly younger and had a shorter duration of symptoms than those in the other groups [Table - 1]. They also had more cognitive (lower MMSE scores) and psychiatric disturbance (higher NPI scores) than the other groups though the groups did not differ significantly in mean dementia severity. As much as two thirds of these patients had gait disturbance and urinary dysfunction while focal neurological signs were seen in about 50% of patients. [Table - 3]. Of the 24 patients with reversible etiologies 20 patients [5 with B12 deficiency, 6 with NPH, 5 with neurosyphilis and one each with cryptococcal and tuberculous meningitis, HIV dementia and neurocysticercosis] were available for follow up which was done until about 1 year. All of these patients had substantially improved with treatment, as shown in [Table - 4]. Discussion Our main finding in this prospective study of patients with dementia is that a high proportion (18%) of dementias is attributable to potentially reversible etiologies. The three most frequent causes of reversible dementia identified in this study are CNS infections, normal pressure hydrocephalus and vitamin B12 deficiency. We could also identify a characteristic clinical profile of dementia caused by reversible etiologies - cognitive impairment with neurologic signs reminiscent of a subcortical pattern of dementia. With appropriate treatment the majority of these patients had improved significantly. The proportion of all dementias attributed to potentially reversible causes was similar to the previous studies.[19], [20], [21] This figure however would have been higher (going up to 30%) had we also included alcohol associated dementia, depressive pseudodementia and surgical causes like brain tumors and chronic subdural hematomas mentioned as potentially reversible in these studies. Recent large studies of reversible dementias from the West have not found CNS infections as causes of dementia.[21],[22] However studies from developing countries such as India[23] and Brazil[24] mentioned neuroinfections especially neurosyphilis as rather coμn. The high prevalence of CNS tuberculosis and neurocysticercosis together with the looming spectre of HIV infection in countries such as India would continue to ensure that neuroinfections reign as coμn causes of reversible dementia in the near future. The relatively younger age of the subjects in these two studies can also explain this difference. That we did not encounter dementia due to thyroid hypo or hyperfunction as mentioned in previous studies [19], [21], [25] is surprising and inexplicable. In our efforts to tease out a characteristic clinical profile of these dementias we found that younger age of onset, shorter illness duration, moderately severe cognitive and psychiatric disturbance and a high frequency of gait disturbance, urinary dysfunction and focal neurological signs could predict a reversible cause with good sensitivity. There has been a similar mention that most reversible causes result in a subcortical pattern of dementia.[26] But the finding of moderate to severe cognitive impairment in dementia due to reversible causes is in striking contrast to the minimal cognitive impairment reported in some of the earlier studies.[19], [21], [25] We deem it appropriate to posit that this could be due to the different mix of reversible causes seen in the present study as compared to others. Also in divergence from results of previous investigations[22],[25] we found that treatment results in substantial improvement (though not amounting to complete reversal) in the majority of such patients. As the length of our follow-up was not more than one year in most patients we would like to adopt a cautious approach before drawing any firm conclusions. The investigative modality that offered maximal diagnostic information independently was CSF examination (routine and serology). In as many as nine patients the final diagnosis could irrefutably be established only by CSF examination (six with neurosyphilis, two with cryptococcal meningitis and one with tuberculous meningitis). Neuroimaging could establish the diagnosis definitively in only one patient with CNS infection (cysticercosis) and helped to avoid lumbar puncture. A few limitations of this study also need to be pointed out. Our results, coming from a specialist clinic of a tertiary referral hospital might not be representative of dementias in the community. But these results might also not be widely off the mark given the burden of malnutrition and infections in the general population. Secondly we do not have autopsy confirmation of the clinical diagnoses of dementias. However strict adherence to well validated criteria could have mitigated some of the inadequacies of clinical diagnosis. Also comprehensive characterization of neuropsychological deficits in patients with reversible dementia could have added more diagnostic information. Lastly it is our view that a higher proportion of patients could have been identified if we had included serum vitamin B12 assay, VDRL and thyroid antimicrosomal antibody estimation in the mandatory laboratory assessment for all patients. We are encouraged along this path by the finding of very high thyroid anti-microsomal antibodies in a recent patient with the clinical picture of posterior cortical atrophy. We still await results of treatment with corticosteroids though. Conclusions Not withstanding the above shortcomings, this investigation has indeed thrown up valuable results that will surely help fine tune the clinical diagnostic approach to dementia. If we have a heightened awareness of neuroinfections and vitamin B12 deficiency as coμn causes of dementia that might be substantially reversible and focus on the particular clinical profile to help direct subsequent investigations, the lessons from this study would have been truly learnt.Acknowledgement The authors would like to place on record their gratitude for Dr.E.Ratnavalli who helped at all stages of this study.References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05100t3.jpg] [ni05100t1.jpg] [ni05100t4.jpg] [ni05100t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}