 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
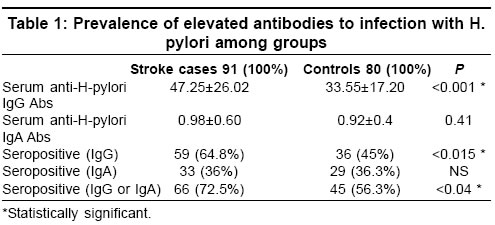
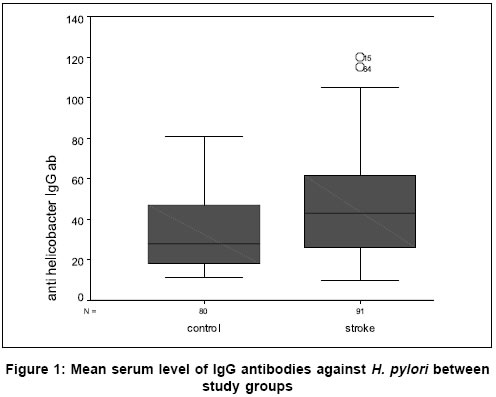
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 303-306 Original Article Association between infection with Helicobacter pylori and cerebral noncardioembolic ischemic stroke Masoud SA, Arami MA, Kucheki E Neurology Department, Shahid Beheshty Hospital, Kashan University of Medical Sciences, Kashan Date of Acceptance: 05-Apr-2005 Code Number: ni05106 Related article: ni05107 Abstract Background: Helicobacter pylori infection has been associated epidemiologically and pathogenetically with atherosclerosis of coronary arteries but data regarding chronic infection with this organism and cerebral noncardioembolic ischemia are not clear. Keywords: Atherosclerosis; helicobacter pylori; ischemic stroke. Helicobacter pylori is notorious for causing chronic infections and has been seroepidemiologically linked to the coronary heart disease and atherosclerosis.[1],[2] Patel et al. found ischemic ECG to be more coμn in men with H. pylori seropositivity with an Odds ratio of 3.82 after adjusting for a range of socioeconomic indicators and risk factors for ischemic heart disease.[3] Murray et al. found that H. pylori seropositive people had 1.51 times more risk of evidence of coronary heart disease according to the Rose angina questionnaire after being controlled for social class and conventional cardiovascular risk factors.[4] Data on chronic infection in cerebrovascular disease are limited. In a pilot study Hugh and coworkers found a significant relation between H. pylori infection and stroke.[5] On the other hand Heuschmann et al. found that chronic H. pylori infection was associated with a higher risk of stroke caused by small-artery occlusion and a lower risk of cardioembolic stroke but totally elevated H pylori antibodies were not associated with ischemic stroke.[6] Because direct detection methods for H. pylori depend on cerebrovascular wall samples retrieved in vivo, which are not available obviously, so antibody levels must be used to describe the association between stroke and previous infection in an indirect manner. Therefore, we have investigated, in a case-control study, whether serological evidence of H. pylori infection is an independent risk factor in noncardioembolic ischemic stroke. In contrast to other studies, we excluded cases with other known risk factors in order to evaluate an independent role of this organism. Patients and methods During a period of one year (2003-2004) all Ischemic stroke patients with following criteria were enrolled in this retrospective analysis study: (a) first ischemic stroke, (b) stroke treatment in a hospital, and (c) admission to a hospital within the first 72 h after stroke onset. Stroke was defined according to World Health Organization criteria. Patients with a known cardiac source for cerebral embolism (Atrial fibrillation, valvular heart disease in echocardiography and prosthetic heart valves), those with major risk factors for atherosclerosis: hypertension, referred to a blood pressure of 140/90 mmHg or greater in repetitive controls; diabetes mellitus, based on American Diabetes Association criteria and any symptoms related to peptic ulcer disease (known peptic ulcer disorder using endoscopy, use of antiulcer treatments, suspected cases according to history and gastrointestinal symptoms), were excluded. Cerebral infarction was diagnosed on the basis of clinical setting and results of the neuroimaging study. Brain CT was done on all patients but, MRI only on the posterior circulation strokes. All patients had abnormal neuroimaging compatible with cerebral ischemic stroke in the certain arterial territory. According to the above inclusion criteria, 91 patients were selected for study. Because patients with lacunar strokes are not hospitalized routinely in our center, only a few cases were lacunar infarctions. Controls selected randomly from general population (hospital workers, individuals who referred our hospital for periodic check up examinations). Controls did not have any history of cerebrovascular and coronary accidents and suspected peptic ulcer disease and matched for age, sex, and area of residence so a total amount of 80 controls could be included in the study. Physical and neurological examination was done for all cases and blood samples were taken within the first week after admission. Information was collected directly from the patient and in case of disability of participant to communicate, from a close relative. Control subjects were interviewed and evaluated in the same manner as cases. Blood samples of either cases or controls were labeled immediately after taking blood. Thus laboratory investigators were blind to case or control status during the laboratory tests. Sera were stored at 2-8°C for 1 week and at 20°C for longer. IgG antibodies to H. pylori were detected using a rapid enzyme linked immunosorbent assay (EIA WELL; REF K5HPG kit; RADIM, Roma, Italia). assay procedure was performed according to the manufacturer′s order and recommended measures were chosen to indicate IgG H. pylori seropositivity. Samples with IgG values less than 15 UR/ml were considered nonreactive for anti-H. pylori IgG antibodies. Values higher than 30 UR/ml were considered reactive and values between 15 and 30 UR/ml considered questionable. According to the manufacturer′s statement, the sensitivity and specificity of the method were 95.8 and 96.2%, respectively. (for more information see: http://www.radim.it) We used Trinity Biotech Captia™. Pylori IgA Enzyme-Linked Immunosorbent Assay kit (USA, ISO 9001 certified, P/N 6430-29 Rev C), for the detection and qualitative determination of IgA antibodies. based on the manufacture′s guide, an Immune Status Ratio (ISR) was calculated for each specimen and ISR values of ≤0.9 was interpreted as negative, 0.91-1.09 as equivocal and retested and ISR values of e ≥.10 analyzed as positive. Relative sensitivity of test with 95% CI is 74.1-100% and specificity of 93.2-100%. (For more information contact: Trinity Biotech USA, Jamestown, NY, Fax (353) 488-1990) Also, the mean levels of each antibody compared between groups. Statistical analyses were performed with the SPSS 11.0 software packet. The t test was used to test differences in quantitative variables, and the c2-test was used to test differences in proportions of qualitative variables. For variables relative risk evaluation we used Odds ratio with a confidence interval (CI) of 95%. Results Total of 91 cases (43 women, 48 men) and 80 controls (40 women, 40 men) were included for analysis (CI 95%, df=1, Fisher Exact Test=0.76). The mean age of patients was 64.3±10 years and of controls was 61.73±10.3 years ( t =1.652, df=169, CI 95%, P =0.1). Seropositivity for antihelicobacter IgG antibody was found in 36 controls and in 59 patients. about IgA type antihelicobacter antibodies, seropositivity was observed in 29 controls (36.3%) and 33 patients (36%) in stroke groups. There was seropositivity for H. pylori (IgG or IgA) in 66 patients (72.5%) but they were positive only in 45 controls (56.3%). [Table - 1] represents a summary of demographic characteristics of cases and controls and prevalence of elevated IgA and IgG antibodies to chronic infection with H. pylori among cases and controls. The mean serum levels of antibodies were analyzed between groups. Mean serum levels of antihelicobacter IgA antibody was 0.92±0.4 in control group and 0.98±0.76 in patients and there was not significant differences between groups ( t =0.824, df=169; CI 95%, P =0.411). Mean of IgG levels was 33.55±17.20 in control group and 47.25±26.02 in noncardioembolic stroke group ( t =4.105, df=169; CI 95%, P <0.001). [Figure - 1] shows our findings. Elevated serum antibodies to H. pylori were significantly associated with a higher risk of noncardioembolic stroke. According to immunoglubin type, this risk was remarkable only for IgG type seropositivity (Odds ratio=2.053; 95% CI, 1.085 to 3.886), but the IgA antibody elevation against H. pylori did not show risk for noncardioembolic ischemic stroke (adjusted Odds ratio=1.001; 95% CI, 0.54 to 1.87). This risk was equal for both sexes. Discussion In our case-control study, IgG antibody response for H. pylori was associated with an increased risk of noncardioembolic stroke. However, no evidence found for any strong association between elevated IgA antibodies to H. pylori and the overall risk of stroke. Because of small sample size, we could not analyze the data according to stroke subgroup. It was the limitation of our study. But in contrast to some previous studies we evaluated definite cases of noncardioembolic strokes. We used numerous exclusion criteria that resulted to a small sample size but we think this relates to robustness strength of our study and results are more definite for evaluation of H. pylori role in noncardioembolic ischemic strokes. Our findings were consistent with the results of the Markus and Mendall study that addressed the relation between chronic H. pylori infection and ischemic stroke.[7] They reported elevated IgG antibodies to H. pylori in the both subgroups of lacunar strokes [Odds ratio 2.21 (95% CI 1.12-4.38), P=0.02] and large vessels strokes with an adjusted OR of 2.58 (95% CI 1.44-4.63, P=0.001), which is compatible with our finding (Odds ratio=2.053; 95% CI, 1.085 to 3.886). Because We excluded cardioembolic ischemic strokes from study, therefore, our findings are consistent with a positive association of chronic H. pylori infection and those ischemic strokes which mainly occurred by an atherosclerotic mechanism of cerebral arteries or other types like lacunar infarction and infarction of unusual cause. Moayyedi et al. in a study on 467 in-patients with clinical evidence of acute ischemic stroke and 388 healthy controls with no evidence of cerebrovascular disease, found a significantly more H. pylori positive individuals in the cases compared to the controls. They concluded (that) infection with H. pylori was associated with an increased risk of stroke and increased fibrinogen levels.[8] Ponzetto and colleague in a similar study evaluated the prevalence of H. pylori infection in 80 consecutive patients with acute ischemic stroke. H. Pylori infection was diagnosed by means of both 13C urea breath test and IgG antibodies to H. pylori also They evaluated H. pylori infection in a group of 320 blood donors matched for sex and age served as controls. The presence of H. pylori infection was higher in patients than in controls: 64/80 (80%) vs 190/320 (59.4%) (P<0.001).[9] Also Grau et al. found H. pylori seropositivity as a possible independent risk factor for stroke of atherothrombotic origin.[10] One study in Argentina demonstrated the presence of the microorganism in carotid lesions. However, they were unable to speculate on the role of H. pylori in the initiation, progression, and/or complication of the atherosclerotic process.[11] Some mechanisms may play a role in atherogenosis of chronic H. pylori infection. These are: a low-grade acute phase response, free radical formation, and immune mediated mechanisms. Blood markers of an acute phase response are raised in chronic H. pylori infection. Free radical formation and immune mediated mechanisms may also be important. Antioxidants have been shown to be decreased in subjects with H. pylori .[12] Another possible mechanism linking H. pylori and atherogenesis is lipid peroxidation due to antioxidants loss.[13] Another explanation about relation between cardiovascular disease and H. pylori is via hyperhomocysteinaemia.[14] There is a potential that chronic bacterial infection may aggravate pre-existing plaque by enhancing T-cell activation as well as other inflammatory responses that may participate in the destabilization of the intimal cap resulting in plaque rupture, progression to acute ischemic syndromes, and ultimate enlargement of the atherosclerotic plaque.[15] Further studies are required to evaluate whether antibiotic treatment may result in clinical benefit to the patients or stroke primary prevention. According to some recent studies, infection with more virulent H. pylori strains, such as cytotoxin-associated gene-A (CagA) bearing strains, may be of particular relevance for ischemic diseases. Preusch investigated whether H. pylori and CagA seropositivity are independent risk factors for cerebral ischemia or its etiologic subtypes. They determined IgG antibodies against H. pylori and CagA protein in 190 patients with acute cerebral ischemia and in 229 age and sex matched control subjects. CagA seropositivity was more coμn in patients (114/190; 60.0%) than in control subjects (99/229; 43.2%; Odds ratio, 1.97; 95% CI, 1.33 to 2.91; P <0.001), which remained significant after adjustment for age, sex, vascular risk factors and diseases, and childhood and adult social status. H. Pylori seropositivity in general was not associated with increased risk of stroke or its etiologic subtypes.[16] Another recent study has shown infection with CagA-positive H. pylori strain in atherosclerotic stroke patients is associated with greater intima-media thickness and poorer short-term outcome compared with CagA-negative patients.[17] Conclusion In summary, our study shows an association between antibody response to H. pylori and first noncardioembolic ischemic stroke. This finding is in accordance with recently published epidemiological studies and meta-analyses on coronary artery and cerebrovascular diseases.[18],[19],[20] According to Cremonini et al., association between H. pylori positivity, anti-CagA positivity and stroke is modest and seems higher with stroke due to large vessel disease.[20] Further studies that are presently ongoing and planned for the near future are expected not only the elucidation of the pathophysiology related to the association between chronic bacterial infection and atherosclerosis but evaluating whether antibiotic treatment may result in clinical benefit of the patient.References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05106t1.jpg] [ni05106f1.jpg] |
| |||||||||

{kind=link}
{kind=link}