 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
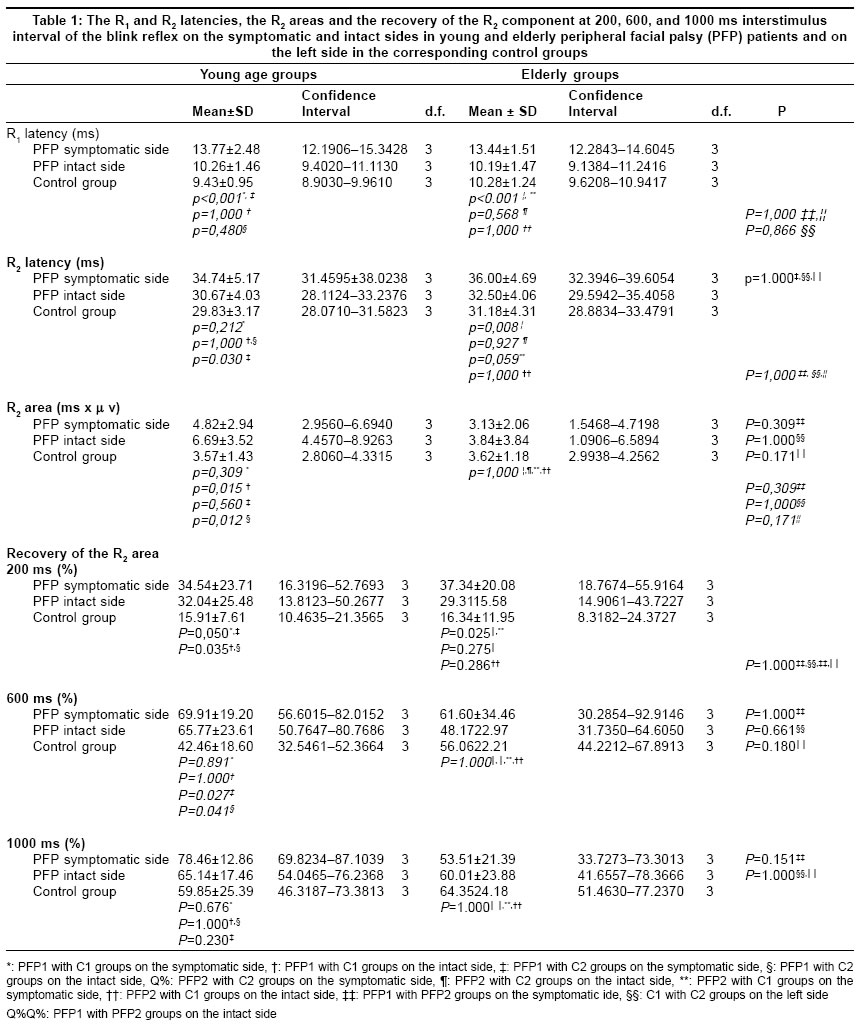
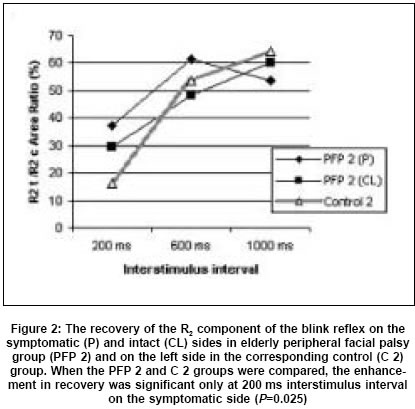
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 318-322 Original Article The influence of age in peripheral facial palsy on brainstem reflex excitability Kiziltan ME, Uzun N, Kiziltan G, Savrun FK Department of Neurology, Istanbul University Cerrahpasa Medical School, Istanbul Date of Acceptance: 26-Mar-2005 Code Number: ni05111 Related article: ni05112 Abstract Background: Neuronal plasticity is expected to be different at different ages and adaptive changes developing after peripheral facial palsy (PFP) may provide a clue in this respect.Aims: To investigate the difference in the reorganization developing after facial nerve damage between patients who developed PFP at childhood-youth and middle-old age. Patients and methods: Twenty-two patients were divided into two groups according to the age-at-onset of PFP; young (PFP 1), and elderly (PFP 2). Two age-matched control groups (C 1 and C 2) comprised of 32 healthy subjects were included in the study. The latency, R2 area, and recovery of the R2 area of the blink reflex were investigated. Statistical analysis : anova and Bonferroni tests were used. Results: The R2 areas were significantly greater on the intact side of the PFP 1 group as compared to that in the control group ( P =0.012). The recovery of R2 component was significantly enhanced on the symptomatic ( P =0.027), and intact ( P =0.041) sides in PFP 1 as compared to that in the C 2 group at the stimulus interval of 600 ms. Significant enhanced recovery was noted at 200 ms stimulus interval on the symptomatic side of the two PFP groups (PFP 1, P =0.05 and PFP 2, P =0.025) and on the intact side of the PFP 1 group ( P =0.035) as compared to that in the control groups. Conclusion : Young age-at-onset of PFP is associated with more prominent excitability changes developing at the neuronal and interneuronal level. Keywords: blink reflex; peripheral facial palsy; recovery of the blink reflex. Motoneuronal excitability changes on the symptomatic and intact sides have been reported after peripheral facial palsy (PFP) in early and late periods.[1],[2] Increased frequency and amplitude of the eye-blink on the intact side or both sides, and later development of blepharospasm in some patients with unilateral PFP may indicate adaptive or maladaptive behavior of the nervous system. [3],[4],[5],[6] Elicitation of the contralateral R1 response following stimulation on the symptomatic side in many cases with unilateral PFP at the regenerative phase was attributed to the synaptic reorganization of the crossing trigemino-facial reflex connections which are functionally suppressed under normal conditions.[7] The changes in the R2 component of the blink reflex (BR) and its recovery following PFP are considered to provide insight to the functional changes occurring after nerve damage in the motor system.[8] The R2 response area of the BR, as an indicator of the excitability of the facial motoneurons, is larger on intact side when the stimulus is applied on the symptomatic side in unilateral PFP, contrary to that found in healthy subjects.[1], [9] PFP can develop at various ages, and one of the factors determining the response of the nervous system to nerve damage is the age-at-onset of the lesion. Therefore, comparing individuals who developed PFP in childhood or youth with those who had developed PFP in middle or old age may provide clues to the influence of age on the reorganization developing after single nerve damage. We studied the area of R2 component of the BR and its recovery in these two groups of patients with unilateral PFP and evaluated the influence of age on the excitability changes at neuronal and interneuronal levels using BR recovery technique. Material and Methods We evaluated retrospectively the EMG recordings of the PFP patients admitted to our EMG laboratory between 2002 and 2004. Patients who have systemic or neurologic diseases, which can affect BR were excluded. The control group consisted of healthy subjects, age-matched with the patient groups. All subjects gave written informed consent to participate in the study after understanding the objectives, and methods of this trial. Local ethical committee was informed of this study and ethical clearance was obtained. Twenty-two subjects with a history of PFP were included in the study. Current ages of the patients at the time of evaluation were between 10 and 69 years, and they developed PFP at the ages between 5 and 66 years. To standardize all parameters except age, only patients with similar PFP durations and clinical presentations were included. All patients had postparalytic overactivity such as synkinesis, and none of them demonstrated persistent complete weakness. Patients were divided into two groups; 12 patients (56%) (12 women) in the childhood-young age group (PFP 1) and 10 patients (45%) (6 women, 4 men) in the middle-old age group (PFP 2). PFP 1 group developed PFP between 9 and 23 (mean 17.1) years of age (mean evaluation age 18.5). PFP developed between 43 and 66 years (mean 55.6) of age in the PFP 2 group (mean evaluation age 57). Mean PFP duration of both PFP groups were 1.5 years. Control group 1 (C 1) (50%) (5 men, 11 women) was comprised of subjects between 16 and 29 years of age, and control group 2 (C 2) (50%) (5 men, 11 women) between 45 and 62 years of age. BR was obtained by electrical stimulation of the supraorbital nerve on both sides with standard methods and it was recorded from both orbicularis oculi muscles, and also from orbicularis oris muscle in order to show synkinetic spread of the reflex response. The cathode was placed over the supraorbital notch. The BR was evoked with a 0.2 ms square-wave pulse at 2.5-3 times the R2 threshold intensity. Upper and lower frequency bands were chosen as 20 Hz and 1 kHz. Input sensitivity was adjusted as 100-200 mV.[10] BRs were obtained using paired pulses delivered at 200, 600, and 1000 ms interstimulus intervals. At least 30-35 s was allowed to pass between each stimulus pair to prevent adaptation. The R2 area was obtained by sweeping the unrectified responses with the area cursor. R2 area was measured within the window from 32 to 90 ms as explained elsewhere.[11] Latencies were read on the screen with the cursor, and the mean of R2 areas of five separate responses obtained randomly were evaluated. Recovery of the R2 area was expressed as a ratio of the mean test R2 to the mean conditioning R2 area. The recordings were performed from symptomatic and intact sides in both PFP patients. Only left sided recordings were obtained in age-matched control patients. The R1 and R2 latencies, the R2 area, and the recovery of the R2 area values of the BR were accepted as dependent variables. Statistical analysis Results We observed synkinetic movements, and spread of the reflex response to the orbicularis oris muscle in all patients. BR latencies R2 areas BR recovery curve Discussion We investigated whether there is a difference in the reorganization developing after facial nerve damage between patients who developed PFP in childhood or youth and those in middle-old age. The R1 latencies on the symptomatic sides of both PFP groups were longer than those in their corresponding control groups as expected. We noted a significant increase in the R2 area, which indicates increased excitability of the facial motoneurons, only on the intact side of the PFP 1 group as compared to that of the control group. Valls-Sole et al. reported increased R2 area on the intact side when the stimulus is applied on the symptomatic side in unilateral PFP.[1], [9] These findings implicate the development of increased excitability of the facial motoneurons on the intact side after unilateral PFP, and our results showed that this phenomenon is more prominent in younger patients. Decreased suppression of the R2 response to the test stimulus using double stimulation paradigm was noted on both sides in the PFP groups. Significant enhanced recovery was reported before on both sides in patients with unilateral PFP.[8] However, the R2 recovery curves obtained in PFP 1 and PFP 2 groups were different in our study. Increased excitability with interstimulus interval of 200 ms was significant only on the symptomatic side in the PFP 2 group, whereas it was significant on both sides in the PFP 1 group. Early recovery of the R2 response is attributed to the increased excitability or decreased inhibition in interneurons, which participate in the formation of this response. It is known that in conditions involving different levels of the motor system recovery of the R2 response is more rapid than normal subjects. [12],[13],[14],[15],[16],[17],[18] In essence, we studied the reflex changes occurring after an axonal damage in the facial nerve, and the extent that these changes are influenced by age. Following an axonal lesion, changes such as an increase in the RNA and growth protein synthesis, accelerated metabolism in neurons, and synaptic stripping in the motor neuron membrane are observed.[19], [20] It has been suggested that these changes may cause a decrease in the control exerted by the central-suprasegmental mechanisms on motor neuron firing, and consequently an increase in motor neuron excitability.[21] In addition to the changes in the neurons, microglial activation and vascular changes associated with reactive astrocytosis in the tissue surrounding the neuron also take place. [22],[23],[24] Hyper-reactivity of glial cells, and the increase in the pro-inflammatory cytokines following destruction was shown to cause decreased efficiency of repair mechanisms associated with aging of the brain tissue. Increased reactivity of astrocytes has been shown following facial nerve axotomy in aged rats as compared to young rats. In the same study, increased glial fibrillary acidic protein was also shown in the facial nucleus contralateral to the lesion side. The mechanism of this contralateral effect could not be explained.[25] Sprouting and reinnervation is more extensive and rapid in the developing central nervous system. Aging was shown to be associated with decreased postlesional sprouting capability in animals.[26] Structural and functional changes in the neuronal elements associated with aging, such as the increase in the basal levels of intracellular calcium, is considered as a form of negative plasticity which lead to the decreased efficiency of neuronal networks to accomplish their complex activities.[27] In conclusion, we have shown that the increased excitability of the BR following PFP follows different patterns in young and elderly subjects. Hyper-reactivity, which may be an adaptive phenomenon, tends to be more intense and bilateral in patients who developed PFP at an earlier age. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05111f2.jpg] [ni05111f1.jpg] [ni05111t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}