 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
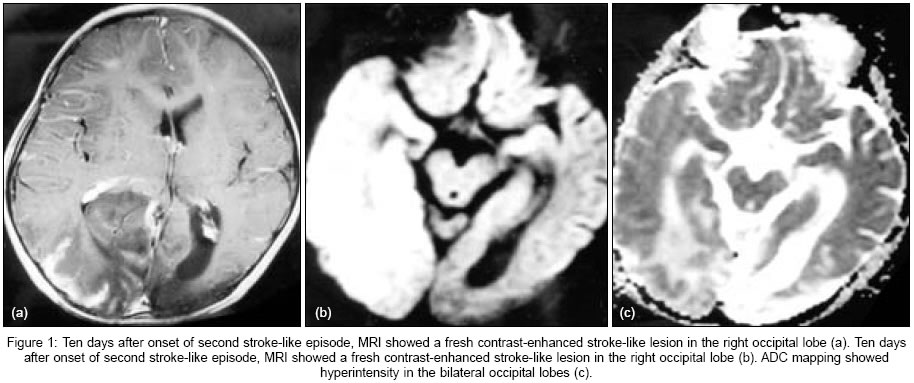
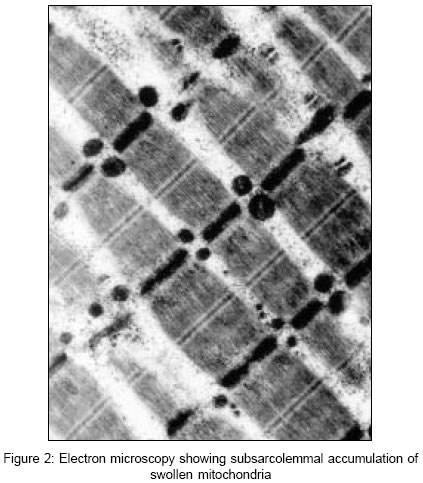
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 323-325 Case Reports Precipitation of stroke-like event by chickenpox in a child with MELAS syndrome Jian-Ren Liu Department of Neurology, Second Affiliated Hospital, School of Medicine, Zhejiang University Date of Acceptance: 01-Mar-2005 Code Number: ni05113 Abstract The mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes syndrome (MELAS) is a rare congenital disorder of mitochondrial DNA (mtDNA). Herein we report a case of MELAS, whose second stroke-like episode was provoked by chickenpox. A point mutation at nucleotide (nt) 3243 in mtDNA supported the diagnosis of MELAS in this case. History of myopathy, the presence of lesions that did not conform to accepted distributions of vascular territories on cranial magnetic resonance imaging (MRI), normal result of cranial magnetic resonance angiography, hyperintensity on diffusion weighted MRI and apparent diffusion coefficient mapping indicating the presence of vasogenic edema in the fresh stroke-like lesion, and mitochondrial DNA analysis helped to exclude the diagnosis of ischemic cerebral infarction which can also be induced by chickenpox.Keywords: Apparent diffusion coefficient mapping; chickenpox; diffusion weighted MRI; MELAS syndrome; stroke-like episode. MELAS (Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes), a syndrome resulting from impaired mitochondrial function, is clinically characterized by nausea, vomiting, encephalopathy, seizures, short stature, headaches, diabetes mellitus, muscle weakness, exercise intolerance, neurosensory hearing loss, myopathy, and sudden neurological deficit.[1] The syndrome is mainly caused by a point mutation at nucleotide (nt) 3243 in mitochondrial DNA (mtDNA). Stroke-like episodes, which always leave new cerebral lesions and deteriorate the illness state and are, thus, the most important clinical characteristic of MELAS syndrome, can be provoked by fever and infections[2],[3]. Herein we report a case of MELAS, whose second stroke-like episode was provoked by chickenpox. In this clinical setting, a differential diagnosis of stroke-like episode of MELAS was considered besides ischemic cerebral infarction, induced by chickenpox. Case History Five days before admission, this then seven-year-old boy had a fever of 38oC and generalized itching maculopapulovesicular rashes, which were umbilicated and dispersed in the face, truck, and proximal extremities. Since thirty-five children in his kindergarten had chickenpox, he was suspected of having chickenpox too. Two days after onset of the rashes, the patient developed headache, vomiting, generalized seizures, and bilateral blurred vision. Four months prior to admission, the patient had an episode of right homonymous hemianopia and recurrent generalized seizures, when the left temporo-parieto-occipital cortex showed an "acute infarction-like" lesion on cranial magnetic resonance imaging (MRI). The patient could not walk until he was three years old. He had muscle weakness and exercise intolerance. However, there was no similar history in the family. Physical examination showed that the patient was alert and had short stature and low body weight. He had body temperature of 37.8oC and normal heart rate, blood pressure, and respiratory rate. Clear vesicular rashes and healing scars were dispersed in the face, extremities, and trunk. The patient could see the movements of the fingers only when they were placed near his eyes. Ocular movements were normal. Gower′s sign was positive. Proximal muscle strength of all extremities was reduced (4+ / 5). Superficial and deep sensations were normal. Plantars were flexor bilaterally. The patient had no aphasia, but his intelligence was subnormal. Results of blood, urine, and stool routine examinations were negative. Serum CPK, AST, ALT, and LDH were mildly elevated, FBS was normal, plasma lactic acid at rest was 11.2 μl/l (normal range 0.7-2.1 μl/l). Test results of protein, glucose, cells, and bacteria in cerebrospinal fluid were normal. Results of electrocardiogram and echocardiogram were normal. Electroencephalograph showed no α activity, but moderate amount of dispersed θ activities (120 m v, 4-6 Hz) and a great deal of pervaded δ activities (120 v, 1-3.5 Hz) in each lead, which were dominant in the right hemisphere. Ten days after onset of the second stroke-like episode, one fresh and one obsolete stroke-like lesion were found in the right and left temporo-parieto-occipital lobes respectively on cranial MRI. The fresh lesion was enhanced by paramagnetic contrast, while the obsolete lesion showed encephalomalacia, cortical atrophy, and ventricular enlargement [Figure - 1]A. Fourteen days after the onset of stroke-like episode, diffusion weighted MRI (DWI) showed hyperintensity in the right occipital lobe (fresh lesion) and hypointensity in the left occipital lobe (obsolete lesion); apparent diffusion coefficient (ADC) mapping showed hyperintensity in bilateral occipital lobes. [Figure - 1]B, C Cranial magnetic resonance angiography (MRA) did not show abnormalities. Gomori′s Trichrome staining of skeletal muscle showed a large number of ragged red fibers, and electron microscopy showed subsarcolemmal accumulation of swollen mitochondria [Figure - 2]. Polymerase chain reaction gene analysis demonstrated a point mutation at (nt)3243 in mitochondrial DNA (mtDNA). The patient was diagnosed as having MELAS preceded by chickenpox and treated with acyclovir, carbamazepine, coenzyme Q, and prednisone. The vesicular rashes disappeared one week later, and the patient was discharged three weeks later when the seizures were controlled and his visual acuity had recovered enough to count the fingers. Discussion MELAS syndrome is characterized by stroke-like episodes, which in turn deteriorate the illness. Stroke-like episodes lead to new lesions in the brain, frequently involving the temporo-parieto-occipital cortex and basal ganglia. Infection can provoke stroke-like episodes in MELAS patients. Sharfstein et al reported a 55-year-old female patient who developed a stroke-like episode during ophthalmic herpes zoster infection.[3] In addition, MELAS may represent an unusual risk factor for certain kinds of infections. McKee et al reported a MELAS patient who had severe infection of the opportunistic fungus Aspergillus fumigatus.[4] In the patient reported here, chickenpox may have provoked the stroke-like episode. Chickenpox was diagnosed according to the manifestation of typical water blisters and clinical history. Since chickenpox can also cause cerebral infarctions in children[5],[6], it was necessary to distinguish stroke-like episode from ischemic cerebral infarction in this patient. He was misdiagnosed as having ischemic cerebral infarction in another hospital when his first stroke-like episode occurred. A detailed clinical history was obtained and upon careful physical examination, we found muscle weakness and exercise intolerance, which raised the possibility of a mitochondrial disorder. Besides history of myopathy, the presence of lesions that did not conform to accepted distributions of vascular territories on cranial MRI, normal result of cranial MRA, hyperintensity on DWI and ADC mapping indicating the presence of vasogenic edema in the fresh stroke-like lesion [7],[8], and mitochondrial DNA analysis helped to exclude the diagnosis of ischemic cerebral infarction in this case. Stroke-like episodes in MELAS syndrome are similar to ischemic cerebral infarction in clinical manifestation and neuroimaging. Clinicians tend to pay more attention to acute neurological deficits and distinct lesions on cranial CT or MRI, and may misdiagnose the stroke-like episode as cerebral infarction. This may occur more often in children, who may be unable to provide a detailed clinical history. A detailed clinical history and physical examination, together with characteristic neuroimaging findings and laboratory data help in making the correct diagnosis of MELAS in children. Acknowledgment Thanks were given to Dr. YUAN Yun for his help of mitochondrial DNA analysis and Dr. ZHOU Fu-You for his help of pathological analysis.References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05113f2.jpg] [ni05113f1.jpg] |
| |||||||||

{kind=link}
{kind=link}