 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
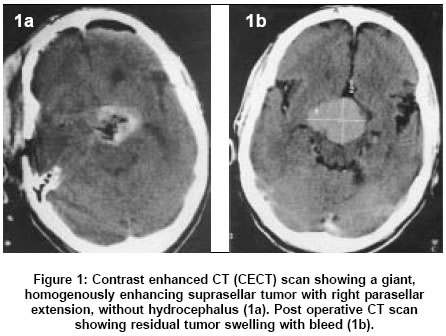
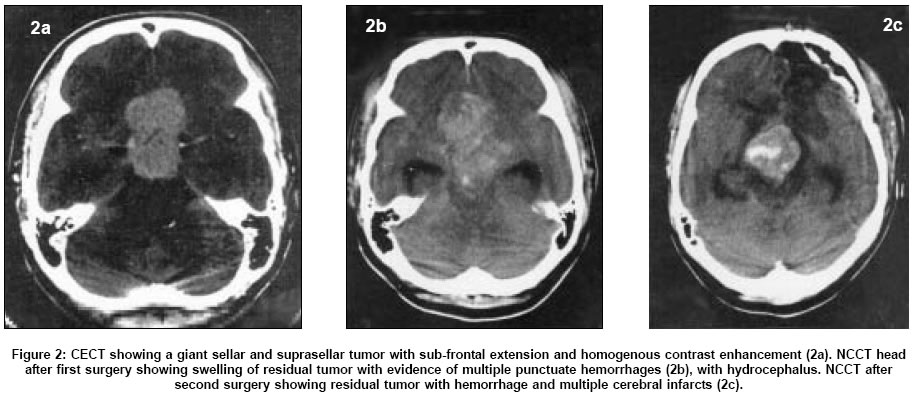
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 326-328 Case Reports Post operative 'pituitary apoplexy' in giant pituitary adenomas: A series of cases Ahmad FaizU, Pandey Paritosh, Mahapatra AshokK Department of Neurosurgery, Neurosciences center, All India Institute of Medical Sciences, New Delhi Date of Acceptance: 15-Mar-2005 Code Number: ni05114 Abstract This is report on four cases of giant pituitary tumors that developed postoperative pituitary apoplexy after they had undergone a partial tumor resection. Three patients had undergone surgery by a transsphenoid route and one patient underwent surgery by transcranial route. Postoperative CT scan showed hemorrhagic expansion of residual tumor mass. All the four patients were re-explored transcranially and hemorrhagic swelling of the tumor was observed. In three cases, the tumor had swollen to a size greater than twice the original tumor. All the four patients had a fatal outcome.Keywords: Giant pituitary tumor, apoplexy, transsphenoid surgery Introduction The phenomenon of postoperative pituitary apoplexy following partial resection of a pituitary adenoma has been described by Goel et al in 1995.[1] In this report we present our experience with four such cases encountered by us in the last 8 years. The high degree of mortality associated with this phenomenon and the implications in pituitary tumor surgical philosophy is discussed[1].Case History In the last 8 years, 890 cases of pituitary tumors were operated at our centre. Among them, 134 patients had giant pituitary adenomas (more than 4 cm in largest extent by definition).[2] Four of these patients developed post operative pituitary apoplexy. Case 1 Case 2 Case 3 and Case 4 Discussion Pituitary apoplexy is a rare and life threatening condition characterized by headache, visual loss, opthalmoplegia, and altered mental status caused by sudden hemorrhage or infarction of the pituitary gland.[3] Massive swelling and hemorrhage in a pituitary tumor or the phenomenon of ′postoperative pituitary apoplexy′following a subtotal or a partial resection of giant pituitary adenomas was described by Goel et al in 1995.[1] Our literature search did not reveal any other report of a similar clinical finding, and it appears that probably this complication is under-reported. All the four patients in our series and in the series reported by Goel et al,[1] the patients had giant pituitary tumors. There was postoperative worsening in the neurological status in all the four reported cases. There was no evidence of alteration of coagulation parameters. Case 1, 2 and 4 had deterioration in sensorium and Case 3 developed third nerve paresis along with visual decline. Despite the decompression of the haemorrhagic tumor during the re-operations, all the patients had a stormy post operative course and subsequently died. Various causes have been postulated for pituitary apoplexy. Some authors have proposed that a rapidly growing adenoma that outstrips its blood supply may lead to ischemic necrosis of the gland.[4] Others propose direct compression of the pituitary infundibulum by an expanding mass, thus compromising the blood flow from the portal vessels, resulting in necrosis of the entire gland with hemorrhage as a secondary occurrence. Sudden release of tumor vessels from the internal carotid artery due to reduced tumor burden and compromise of the venous drainage of the tumor during surgery have also been proposed.[1] Tumor manipulation during surgery, swelling and subsequent compression of the hypophyseal arteries causing hemorrhagic necrosis is a plausible explanation in our cases. However Cardoso and Peterson[5] did not agree with the above theory since angiographic studies show that pituitary adenomas derive their blood supply from inferior hypophyseal arteries and not from superior hypophyseal arteries, which get compressed with the impaction of the enlarging tumor against the diaphragmatic notch. Lath and Rajshekhar reported a patient who died of massive cerebral infarct due to direct compression of the internal carotid artery caused by pituitary apoplexy.[6] Hypothalamic disturbances could be an important cause of mortality in such cases and at least one of our cases (Case 2) had evidence of hypothalamic dysfunction. It has been proposed that a radical tumor resection must be attempted during the first surgery for giant pituitary adenomas [1],[2]. Our experience and that of others suggest that surgery for giant pituitary adenomas is a formidable surgical challenge.[1],[7] References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05114f1.jpg] [ni05114f2.jpg] |
| |||||||||

{kind=link}
{kind=link}