 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
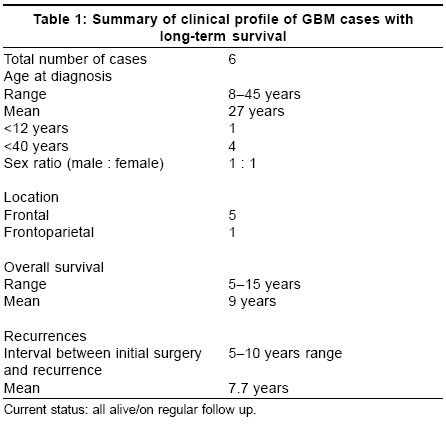
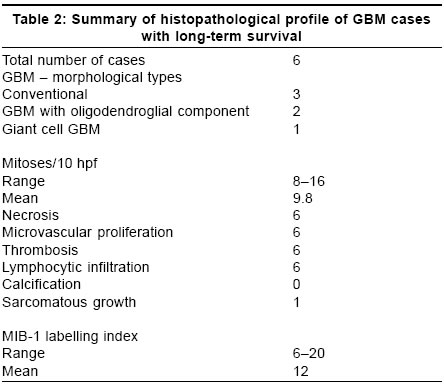
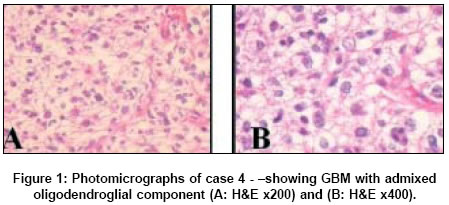
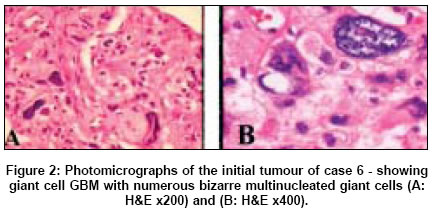
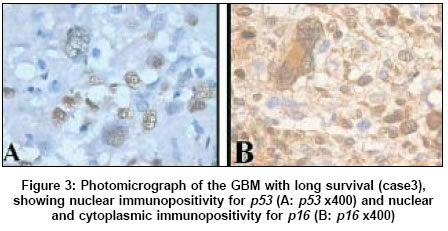
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 329-332 Case Reports Glioblastoma multiforme with long term survival Deb Prabal, Sharma MeharChand, Mahapatra AshokKumar, Agarwal Deepak, Sarkar Chitra Departments of Pathology, All India Institute of Medical Sciences, New Delhi Date of Acceptance: 30-Mar-2005 Code Number: ni05115 Abstract Glioblastoma multiforme (GBM) Patients generally have a dismal prognosis, with median survival of 10-12 months. GBM with long-term survival (LTS) of ≥ 5 years is rare, and no definite markers indicating better prognosis have been identified till date. The present study was undertaken to evaluate GBMs with LTS in order to identify additional correlates associated with favourable outcome. The cases were evaluated for relevant clinicopathological data, proliferation index and expression of tumortumour suppressor gene ( p53 ), cyclin-dependant kinase-inhibitors ( p27 and p16 ) and epidermal growth factor receptor (EGFR) proteins. Six cases of GBM with LTS with an average survival of 9 years (range 5-15 years) were identified. All were young patients with mean age of 27 years (range 8-45 years). Histology of three cases was consistent with conventional GBM, while two showed prominent oligodendroglial component admixed with GBM areas. One was a giant cell GBM, which progressed to gliosarcoma on recurrence. The mean MIB-1LI was 12% (range 6-20%). p53 was immunopositive in 4 out of 5 cases. EGFR and p27 were immunonegative in all, whereas p16 was immunonegative in 3 out of 5 cases. Currently, in the absence of specific molecular and genetic markers, GBM in young patients should be meticulously evaluated for foci of oligodendroglial component and/or giant cell elements, in addition to proliferative index and p53 expression, since these probably have prognostic connotations, as evident in this study. The role of p16 and p27 however needs better definition with study of more number of cases. Keywords: Glioblastoma multiforme, long-term survival, favourable outcome Introduction Glioblastoma multiforme (GBM) are generally associated with a poor prognosis, with median survival of 10-12 months.[1] 5-year survival is rare and is reported to be around 4-5% only.[2],[3] Owing to the paucity of GBMs with long-term survival (LTS), no definite picture has emerged till date, though a number of clinical,[4] histopathological[5],[6] and molecular markers[5],[7],[8] have been associated with favourable prognosis. It was aimed to evaluate GBMs with LTS for their distinctive clinical features, histopathological profile, proliferation index and expression of tumour suppressor gene ( p53 ), cyclin-dependant kinase (cdk)-inhibitors ( p27 and p16 ) and epidermal growth factor receptor (EGFR) proteins, in order to identify any additional correlates associated with LTS. Case series Out of a total of 1296 cases of GBM diagnosed during 1989-1999, 6 cases (0.5%) with survival ≥ 5 years, were selected from the records. Clinical profile [Table - 1] Histopathological evaluation In case 6, special stains for reticulin (Gomori-Sweet silver stain) and Masson′s trichrome, as well as IHC using monoclonal antibodies to vimentin (1:50, Novacastra), CD 34 (1:300, Dakopatts), Desmin (1:15, Dakopatts) and smooth muscle actin (SMA - 1:15, Dakopatts) were done. Proliferation index was evaluated using MIB-1 antibody (1:200, Dakopatts), and manually counting 1000 cells from at least 5 representative microscopic fields, at high power magnification (400x). Histopathological features [Table - 2] Case 6 was a giant cell GBM (GCG), with two recurrences at 8 and 9 years after initial surgery. Morphology at initial surgery and first recurrence was that of GCG [Figure - 2]A,B characterized by monstrous multinucleated giant cells with abundant eosinophilic cytoplasm and a reticulin-poor morphology. Biopsy at second recurrence showed a gliosarcoma with distinct GFAP-immunopositive giant cell GBM areas, and reticulin-rich GFAP-immunonegative sarcomatous areas composed of densely packed long bundles of spindle cells, with nuclear atypia and high mitotic activity. Immunostaining for CD34, SMA and desmin were however negative in both the initial and recurrent tumours. Mitoses ranged from 8-16/10 high power field (hpf) (mean 9.8/10 hpf). MIB-1 LI Expression of oncogene / tumour suppressor gene protein However, all the cases were immunonegative for EGFR and p27 . Follow up Discussion Till date, little data is available regarding GBM patients with LTS (≥ 5 years). Scott et al [7] analysed 689 GBMs and confirmed only 2.2% to have LTS, while, McLendon et al[2] detected 2% GBM with LTS among 766 cases. Recently, Shinojima et al[4] reported 6 such cases (5%) out of 113 adult patients with GBM. However, this study analysed the first such data in India and observed an incidence of only 0.5%. On analysing the available literature, it was observed that clinical parameters like young age,[1] predominance of female sex,[4] aggressive surgical resection and a good Karnofsky performance score[5] in GBM are generally associated with better prognosis. Similarly, in the present study cases were young (mean age 27 years), lacked a male predominance and had undergone gross total resection. This was however different from that observed in conventional GBMs. Typically, the histological predictors of better outcome in GBMs include presence of giant cells,[2],[4],[6] focal oligodendroglial differentiation,[2] absence of small anaplastic cells[2] and evidence of better differentiation with more GFAP positivity,[5] all of which were evident in the present series. GBMs with LTS characteristically demonstrate a lower proliferation index (MIB-1LI 5.7%)[8] as compared to the WHO recommended levels of 15-20% for conventional GBM.[1] Overall, the proliferative activity in the present series was 12% (range 6-20%), which was not only lower than the WHO[1] recommended level, but was also substantially lower than the mean cut-off level (22.09±14.73)[9] for conventional GBMs in this laboratory. Although a number of molecular markers have been studied for prognostication in GBMs, only a combination of LOH 1p and 19q defined GBM patients with a significantly better survival.[5] However, Burton et al[8] evaluated the largest sample size of GBM with LTS and observed differences in the rate of abnormal p53 expression (85%), when compared with tumours from a cohort of patients with similar age and KPS but with poor survival. In the present study, p53 was immunopositive in 4/5 cases, while that for conventional GBMs at this centre ranged from 43-61% (mean 50%).[10] Though these observations suggest that the LTS group may possibly represent a different subgroup of GBMs with favourable outcome, further evaluation with more number of cases is warranted for a definite opinion. Burton et al[8] evaluated EGFR as a prognostic marker in gliomas, and observed over expression in 12% of GBMs with LTS as compared to 25% of conventional GBMs. This difference was not statistically significant, and hence no consensus has been reached in regard to its significance.[8] A recent study by Heimberger et al[11] has reported EGFR over expression in 50-60% of GBM, while the most coμn mutant EGFRvIII expression in 24-67% cases, but failed to find a correlation with overall survival. However, in cases surviving >1 year, EGFRvIII was an independent negative prognostic indicator. In the present study all cases were immunonegative for EGFR and hence were non-contributory. Schmidt et al[5] observed LOH 1p/19q in 5 cases of primary GBM, which did not exhibit any areas of oligodendroglial differentiation, but had a significantly better survival. Since all the cases in the present study were possibly de novo GBMs (with no clinical or histopathological evidence of progression from low-grade astrocytomas) with a better survival, molecular evaluation with LOH 1p/19q studies, becomes imperative to exclude foci of oligodendroglial alterations in the remaining cases (omitted owing to lack of facility in this centre). Studies with cyclin-dependant kinase-inhibitors ( p16 and p27 ) have concluded that loss of p16 apparently plays a definite role in glioma progression,[12] while low p27 correlates with high-grade tumour, and predicts poor outcome.[13] In this series p16 was immunonegative in 3/5 cases, which was apparently comparable to that reported for conventional GBMs,[12] p27 immunonegativity with favourable outcome may possibly indicate that LTS cases are a separate subset of GBM, which is independent of p27 inhibition. Interestingly, a gliosarcomatous transformation was observed in the giant cell GBM, which is the first such case reported in literature. This possibly represents mesenchymal metaplasia of GBM cells,[14] rather than a separate neoplasm, which is further substantiated by the presence of p53 immunopositivity in both the glial and sarcomatous areas. A vascular smooth muscle origin of the sarcoma was however ruled out by the absence of CD34 and SMA markers. To conclude, the factors that possibly led to long-term survival in the present series could be younger age, female sex and aggressive surgical resection, in conjunction with features like focal oligodendroglial component, giant cell GBM, lack of small anaplastic cells and a low proliferation index with high p53 immunopositivity. However the role of p27 and p16 immunonegativity needs better definition with study of more number of cases. This study reflects that LTS patients possibly represent a complex subset of GBMs, which cannot be characterized by a single parameter, and warrants further genetic studies. Until then, histopathologists should carefully assess GBM in young patients for foci of oligodendroglial component, giant cell elements and areas with extensive GFAP reactivity, as well as proliferative index and p53 expression, since these appear to have prognostic connotations. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05115t2.jpg] [ni05115t1.jpg] [ni05115f2.jpg] [ni05115f1.jpg] [ni05115f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}