 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
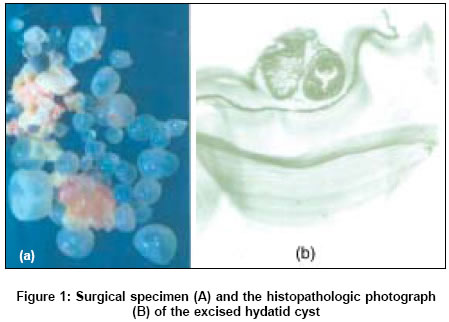
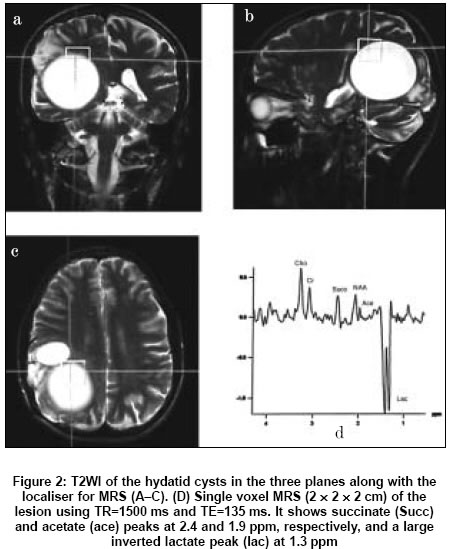
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 337-338 Case Reports In vivo proton magnetic resonance spectroscopy in a known case of intracranial hydatid cyst Chand K, Kanodia AK, Manpreet G, Neeraj A Department of Neuroradiology, IHBAS, Delhi Date of Acceptance: 11-May-2005 Code Number: ni05118 Abstract We are presenting magnetic resonance spectroscopy (MRS) findings of a known case of hydatid cyst operated twice in the past. A 22-years-old male patient had presented with recurrent symptoms of generalized seizures and raised intracranial tension. MRI with MRS of the lesion was performed that showed a recurrent loculated cystic lesion in right parieto-occipital lobe. MRS through the lesion was performed using repetition time (TR) of 1500 ms and time to echo (TE) of 135 ms using 2 x 2 x 2 cm voxel, from the margin of the lesion. MRS showed mildly elevated choline (Cho), depressed creatine (Cr) and N-acetyl aspartate (NAA), a large peak of lactate, pyruvate and acetate peaks. Keywords: Hydatid; magnetic resonance spectroscopy (MRS); pyruvate. The differential diagnosis of intracranial brain lesions, including malignant lesions as well as a wide range of benign lesions such as abscesses, can be at times difficult even with the most sophisticated imaging techniques.[1] This is particularly true in case of rare lesions, such as hydatid cysts. Any modality that can hint towards a particular diagnosis cannot only result in optimum conservative or surgical management, but an unnecessary biopsy may be prevented. It is in this context that proton magnetic resonance spectroscopy (MRS) helps as an auxillary method to identify the nature of some encephalic lesions.[2] Proton MRS provides a noninvasive method for examining a wide variety of metabolites in the human brain, including N-acetylaspartate (NAA), choline (Cho), phosphocreatine and creatine (Cr), lactate (Lac), lipids and others such as succinate, pyruvate, aminoacids, acetate, glycine, glutamine/glutamate and inositol.[3],[4] Only some case reports are present in the literature showing proton MRS findings in hydatid cysts.[5],[6],[7],[8] We present MRS findings in this operatively proven case of hydatid cyst of the brain. Case report A 22-year-old man was operated for right parieto-occipital multiple intracranial hydatid cysts 4 years back. He had presented with raised intracranial pressure and generalized seizures. The diagnosis was confirmed histopathologically [Figure - 1]. The patient was given albendazole for 3 months. Postoperative CT scan done 1 month after surgery had revealed no residual cysts. The patient made good recovery and was asymptomatic till 5 months back when he again presented with recurrent generalized seizures and raised intracranial pressure. Repeat CT head revealed recurrent multiple hydatid cysts in the right parieto-occipital lobe. The patient was reoperated 5 months back. He again made good recovery after surgery and is being continued on albendazole and anti-convulsants. A recent MRI showed a residual/recurrent loculated cystic lesion in the right parietal lobe without any perifocal edema [Figure - 2]. We performed proton MRS through the margin of the lesion using single voxel PRESS technique using the following parameters; TR = 1500 ms, TE = 135 ms, NEX = 256, voxel size = 2 ´ 2 ´ 2 cm [Figure - 2]. Prior to the acquisition, localized shimming at the region of interest (ROI) was performed, followed by water suppression adjustment. After zero-filling and baseline correction, peak integrals were calculated by line fitting. Cho peak at 3.2 parts per million (ppm) was increased, the Cho/Cr ratio being 1.64. A NAA peak at 2 ppm was also depressed, the NAA/Cr ratio being 0.85. In addition, a large inverted bifid Lac peak, and small peaks at 1.9 and 2.4 ppm were observed presumed to be acetate and succinate peaks. The patient is waiting for surgery again. Discussion Proton MRS is widely used both as a clinical and research tool, in the evaluation of benign and malignant lesions of the brain. A few case reports and studies mention the role of MRS in hydatid cysts.[5],[6] Since the present case is a proven case of hydatid cyst, we thought it worthwhile to perform MRS in this case. We found metabolites at 1.9 and 2.4 ppm, likely to represent acetate and succinate. These are well-known metabolic end-products arising from micro-organisms.[1] There has been some confusion in the literature relating to the peak at 2.4 ppm as succinate or pyruvate. Most studies assign it to succinate[7],[8] while a few other ones to pyruvate,[5],[6] which mention pyruvate, as a specific in vivo marker for cestodal cysts, hydatid in particular. Succinate is not specific for hydatid cyst and is seen in other parasitic diseases like neurocysticercosis (NCC) as well in abscesses.[9],[10] In addition, acetate is known to be present in parasitic cysts and bacterial abscesses although in abscesses, the acetate peak is higher than succinate, while the reverse is true for NCC and hydatid.[11],[12],[13] In all previous case reports, acetate was present in the hydatid cysts. We observed a large Lac peak at 1.3 ppm. Lac is a product of anaerobic metabolism, and is a nonspecific marker. Almost all studies show it to be present in bacterial abscesses and parasitic cysts. A small peak of NAA was observed. This is attributed to the surrounding brain parenchyma that was included in the voxel. A small Cho peak was also observed, but it is a nonspecific marker, and can be found is almost all benign and malignant lesions, except when spectrum is obtained from the core of the cyst, when it is usually reduced. In addition, the laminated membranes of hydatid cysts are known to be composed of Cho containing compounds.[8] A few previous studies[5] have also shown the presence of alanine in hydatid cysts which we did not find in our case. The MRS of the present case shows that relatively specific spectra may be present in cases of hydatid of the brain. In vivo MRS may be used as an adjunct in the diagnosis of intracranial hydatid cysts. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05118f1.jpg] [ni05118f2.jpg] |
| |||||||||

{kind=link}
{kind=link}