 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
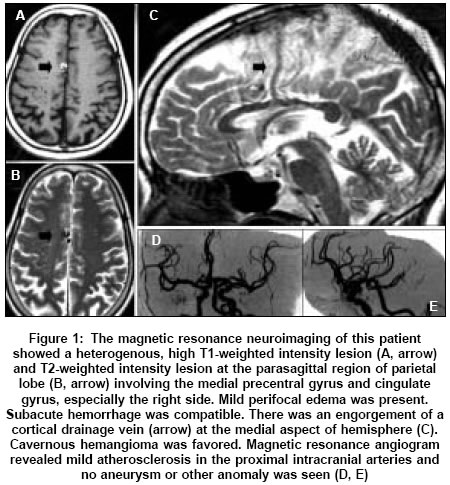
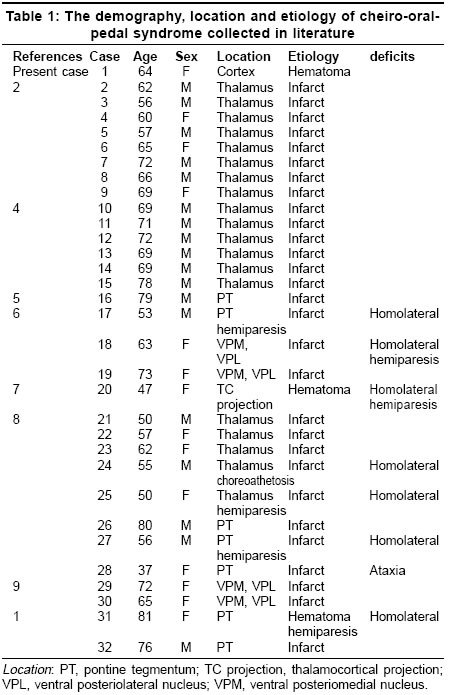
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 342-344 Case Reports Parasagittal hemangioma associates with unilateral cheiro-oral-pedal syndrome Lin HungSheng, Lui ChunChung, Chen WeiHsi, Liu JiaShou Departments of Neurology and Neuroradiology, Chang Gung Memorial Hospital, Niao Sung Hsiang Date of Acceptance: 07-Jun-2005 Code Number: ni05120 Abstract Cortical lesion might elicit restricted acral sensory deficit but a disparity of topographies in cheiro-oral-pedal syndrome is very rare. We report the first case of cheiro-oral-pedal syndrome due to a contralateral parasagittal hemangioma involving the supplement sensory area in parietal lobe. This unusual link between neuroanatomy and neurological feature is discussed.Keywords: Cheiro-oral-pedal syndrome, parietal lobe, hemangioma, sensory Introduction Cheiro-oral-pedal syndrome (COPS) is a sensory disorder, firstly reported in 1992 by Yasuda et al,[1] restricted to the homolateral perioral region, fingers/hand and toes/foot. Till now, only a limited number of COPS patients have formally been reported in literature.[2] The COPS usually arises from an involvement of the ascending spinotrigeminothalamic tract at thalamus and less, pons or thalamocortical projection. [2] Two questions are still whirling in this sensory disorder. First, the involved body parts separate distantly. Second, the paroxysmal relapse of sensorum in COPS is substantially unknown. We encountered a woman with an unusual cortical lesion presenting with COPS. The mechanism is discussed.Case history A 64-year-old hypertensive woman received antihypertensive treatment regularly more than 20 years. However, episodic concurrence of palpitation, anterior chest tightness, neck soreness and an elevation of systolic blood pressure over 200 mmHg in spontaneity occurred 2 years ago. Initially, the frequency was once in every 2 to 3 months and the duration was less than 15 minutes. One week before admission, the frequency of these events increased to daily basis. Meanwhile, a new onset of numbness confined to her mouth angle, hand and foot also developed. Her numbness was accompanied with an elevation of systole over 160 mmHg every time. It lasted for 5 minutes, subsided, and then recurred over 4 to 5 times daily. Five days later, her numbness became persistent without recovery. She denied having familial disease, diabetes mellitus, migraine, recent head injury, toxic substance exposure nor consumption of herb, illicit drug, beverage or cigarette. On presentation, her vital signs were stable. She was conscious and oriented. Her speech and cognition were normal. Pupils were isocoric and reactive, and their sizes were 3.0 mm/3.0 mm. Visual acuity was 20/20 and visual field was not limited. Neuro-ophthalmology, cranial nerves, motor function, co-ordination and equilibrium were normal. Corneal reflex was intact. Pinprick pain and cotton fine touch sensation decreased mildly (10%) at the left hemibody, but densely (80%) at the perioral region, fingers, hand, and foot. Vibratory sense and joint position sensation were intact. Cortical sensation decreased 20% on left side. COPS was interpreted. Head magnetic resonance image revealed a heterogenous, high T1 and T2-weighted intensity lesion at the parasagittal region of parietal lobe involving the medial precentral gyrus and cingulate gyrus, especially the right side [Figure - 1]. Supplementary sensory area was involved. Mild perifocal edema was present. Subacute hemorrhage was considered. An inhomogenous uptake of contrast within the lesion was seen. An engorgement of a cortical drainage vein at the medial aspect of hemisphere was also noted. Cavernous hemangioma was favored. Magnetic resonance angiogram revealed mild atherosclerosis at proximal intracranial arteries. Electroencephalogram did not show any paroxysmal discharge during sensory attack. Somatosensory evoked potential did not reveal any abnormal change of amplitude or latency at median and peroneal nerve stimulation. Biochemistry, hematology, serology, urinalysis, cardiac function and stroke risk factor survey [3] were normal. During hospitalization, her COPS exacerbated when systole increased to over 180 mmHg. The severity of sensorum decreased following with a reduction of arterial blood pressure. She and her family refused any further investigation and treatment. Her numbness progressively subsided within one month without topographic sequence. On a follow up of 6 months, she was uneventful and her blood pressure was controlled well. Discussion To our knowledge, this patient is the first report of COPS associated with cortical lesion. Till now, there are a total of 31 COPS patients reported in literature [Table - 1].[1]-[2], [4],[5],[6],[7],[8],[9] Including our patient herein, they are 18 men and 14 women. The age ranged from 37 to 81. Over 53 % patients were older than 65 years. Thalamus is involved in 23 out of 32 patients, following by pons in 7 and thalamocortical projection in another 1 patient, respectively [Table - 1]. Our patient is the only one to have cortical lesion. A close proximity of the ascending tracts from the perioral region, fingers/hand and toes/foot could explain the characteristic picture of COPS in subcortical but not cortical level. A low prevalence of cortical involvement in COPS may reflect a more distant disparity of the representation areas of perioral structure, fingers/hand and toes/foot in sensory cortex than the cheiro-oral syndrome. Currently, at least five hypotheses have been proposed for the occurrence of cheiro-oral syndrome but they do not fully explain this peculiar sensory disorder: [10] (1) epileptogenesis was suggested in prior but an absence of paroxysmal discharge and change of pituitary hormones in ictus discarded this possibility; (2) migraine is less likely as the time onset, clinical picture, age of onset, and an absence of aura or headache during sensory attack do not support this consideration; (3) an unusual dual vascular supply has been proposed but cannot be confirmed; (4) a preconditioned neuronal vulnerability is only illustrated in cortical motor neuron but not cortical sensory neuron; (5) a combination of the above proposals has been suggested but there is no evidence to support. In our patient, a link was seen between an overshooting of arterial blood pressure and occurrence of sensorum. A rapidity of relapsing sensory deficit in cases of cheiro-oral syndrome [11] has been described in association with an exacerbation of previous hypertension that is known to render vasoconstriction such as in posterior ischemic leukoencephalopathy syndrome. [12] Therefore, with previous reports and our experience, we believe that a complexity of consequences predicts the unusual occurrence of COPS. We propose that a pre-existing brain damage (old age, high frequency of cardiovascular risk factors) and a preconditioned neuronal vulnerability, if under vascular compromise (low perfusion, stroke, brain tumor and others), might provoke this peculiar sensory deficit in cortical level. The paroxysm is probably a result of vascular compromise. COPS is an incomplete pure sensory syndrome, which mostly results from lacunar stroke, stabilizes rapidly after onset and recovers favorably.[13] From our patient, a concomitant nonsensory neurological deficit or a fluctuation of sensory syndrome should caution for a nonlacunar course as in our patient. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05120f1.jpg] [ni05120t1.jpg] |
| |||||||||

{kind=link}
{kind=link}