
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 53, Num. 3, 2005, pp. 354-357
|
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 354-357
Technical Report
Surgery for dural ossification in association with cervical ossification of the posterior longitudinal ligament via an anterior approach
Mizuno Junichi, Nakagawa Hiroshi, Song Joonsuk, Matsuo Naoki
Department of Neurological Surgery, Aichi Medical University
Correspondence Address:Department of Neurological Surgery, Aichi Medical
University, Yazako, Nagakute, Aichi, Aichi-gun, jmizuno@amugw.aichi-med-u.ac.jp
Date of Acceptance: 25-Jun-2005
Code Number: ni05125
Abstract Study design : Direct removal of an ossified mass via an anterior approach carries good decompression, to one- or two-level ossification of the posterior longitudinal ligament (OPLL) of the cervical spine. Ossification occasionally involves not only the posterior longitudinal ligament (PLL) but also the underlying dura mater. Defect of the dura mater by resection of the dural ossification (DO) can cause cerebrospinal fluid leakage or neural injury. The technique of resection of OPLL with floating of DO provides satisfactory decompression and avoids dural defect or neural injury in OPLL associated with DO.
Methods: Four patients developed cervical myelopathy. Radiological examination revealed cord compression due to OPLL associated with DO.
Results: All patients underwent anterior procedures. After the necessary discectomies and corpectomies, OPLL was resected using a high-speed drill with a 4-mm steel burr and then with a 4-mm diamond burr. When the OPLL became paper-thin, it was separated from the dura mater using a microdissector and a Kerrison rongeur. There was a thin layer of the nonossified degenerated PLL between the residual OPLL and DO. Meticulous dissection of the residual OPLL over the DO was performed without removing the DO at this layer. Fixation was performed with a titanium cylindrical cage.
Conclusion : This technical note describes the successful decompression of the spinal cord by removing OPLL only, and avoidance of dural defect or neural injury in cases of OPLL associated with DO.
Keywords: Anterior cervical approach; dural ossification; ossification of the posterior longitudinal ligament; surgery.
Ossification of the posterior longitudinal ligament (OPLL) is one of the major diseases in which cervical myelopathy or radiculopathy develops. [1],[2],[3],[4],[5] Various operative procedures using either an anterior approach or a posterior approach have been used for treating this disease. Anterior approach is essentially performed in cases of one- or two-level segmental OPLL or hypertrophied posterior longitudinal ligament (PLL) with or without associated intervertebral herniated discs, while multilevel laminectomy or laminoplasty is indicated for continuous or mixed-type OPLL. [6],[7],[8],[9],[10],[11] Although anterior decompression of the spinal cord by resection of the ossified ligament combined with anterior arthrodesis can achieve more satisfactory results than posterior approach, surgical tactics are of importance to avoid unexpected complications including cerebrospinal fluid (CSF) leakage and spinal cord damage. [12],[13],[14] Because OPLL is known to involve ossification of the dura mater or to be tightly adherent to the dura mater, unexpected dural, arachnoidal, or underlying neural injury by removing the entire ossified mass may occur, resulting in neurological compromise as well as CSF leakage.[12],[15],[16] We describe a surgical technique for dural ossification (DO) associated with OPLL, for achieving satisfactory decompression and for avoiding intraoperative complications in anterior procedures.
Case reports
Patient 1
A 61-year-old man fell down, and suddenly felt weakness in his right arm. An examination revealed 4/5 strength in his right wrist extension, hypesthesia in the right C6 and C7 areas and deep tendon hyper-reflexes in his knee and ankle jerks. Imaging studies revealed segmental OPLL at C4-5 and C5-6 and DO at C4-5. A diagnosis of segmental OPLL with associated DO was made. He underwent anterior approach for decompression and fusion at the two levels. After necessary discectomies and corpectomies, removal of the OPLL using a high-speed drill was performed until the PLL was revealed between the OPLL and DO. The ossified portion of the dura mater was then floated. After confirming good pulsation of the dural theca, anterior fusion with titanium interbody cages was performed. The patient showed good recovery postoperatively with improvement of his neurological status.
Patient 2
A 71-year-old man developed numbness in his upper extremities. A neurological examination revealed hypesthesia in the C6, C7, and C8 areas bilaterally. Imaging studies revealed segmental OPLL at C4-5 and associated DO at C5-6, causing cord compression. Anterior procedures were performed. After a necessary corpectomy, OPLL was drilled out with a high-speed drill until the underlying PLL was exposed. When the OPLL was removed, the dura mater with the ossified portion showed good bulging and pulsation. Postoperative X-rays revealed a floated DO. The patient numbness became mild.
Patient 3
A 57-year-old man fell down on the road. After this episode,
he felt dysesthesia in his left arm. A neurological examination
revealed 2/5 strength in his left deltoid and biceps, 3/5 strength
in his left triceps, and hypesthesia in the left C6 area. Imaging
studies revealed segmental OPLL at C4-5 and C6-7 and OPLL with
DO at C5-6, with cord compression. Direct removal of OPLL using
a high-speed drill was performed without removing the DO. Meticulous
separation of the OPLL from the ossified dura was performed, however,
slight dural laceration occurred. After decompression, the dura
mater showed good pulsation. The dura was repaired by placing fascia
covered with fibrin glue. Postoperative computed tomography (CT)
revealed a floated DO. The patient showed reasonable improvement
of the neurological status postoperatively.
Patient 4
A 58-year-old man developed painful numbness in his
left arm 2 years ago. A neurological examination showed
3/5 strength in
his left deltoid and 4/5 in his left biceps, hypesthesia in the
left C5 and C6 areas and increased deep tendon reflexes in the
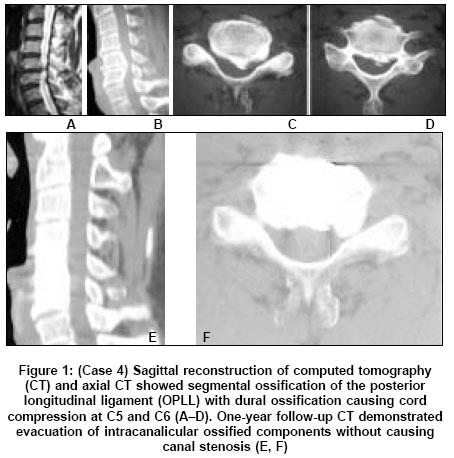
knee and ankle jerks. Sagittal CT reformation revealed a double-layer
ossification at C5-6, and magnetic resonance (MR) imaging demonstrated
cord compression at the same level. Anterior approach with direct
removal of OPLL combined with interbody fusion was performed
at C4-5 and C5-6. The ossified portion of the dura mater
was not drilled.
Postoperatively, the patient showed good recovery. Postoperative
sagittal CT reformation revealed evacuation of OPLL as well as
DO [Figure - 1].
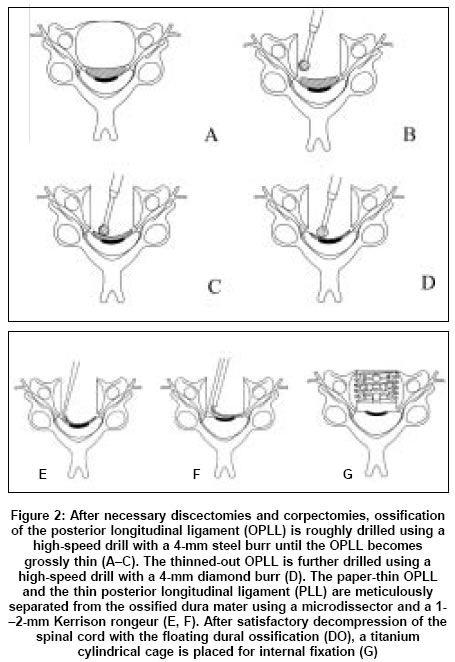
Surgical technique
The patient is placed in the
supine position with the head slightly
extended [Figure
- 2].
A transverse skin-fold incision is made, beginning at the midline
and crossing the anterior border of the sternocleidomastoid
muscle. The appropriate surgical
level is confirmed by intraoperative
portable radiography. After necessary discectomies,
the
vertebral bodies
(VBs) are partially removed using an appropriate reamer. The
residual VBs are removed using a high-speed drill.
When the underlying OPLL
is exposed, a high-speed drill with a 4-mm cutting burr is
used for gross thinning of the OPLL.
After the OPLL becomes thin,
the head of the high-speed drill is changed from a
steel burr to a
diamond burr. The residual OPLL continues to be drilled until
it becomes paper-thin. Then, the OPLL is meticulously
separated from
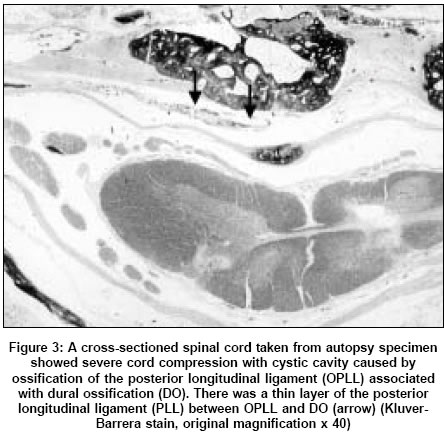
the underlying dura mater using a microdissector. There is
a thin layer consisting a nonossified
degenerated PLL between
the OPLL
and the ossified portion of the dura mater [Figure
- 3].
The residual thinned-out OPLL and the PLL over DO are resected
from the dura mater and its ossified portion using a microdissector
and a small Kerrison rougeur. The ossified portion of the dura
mater is left alone to avoid dural defect and CSF leakage.
After the OPLL is removed, the dura mater becomes bulged and
shows
good pulsation. Hemostasis is achieved by an electrical cautery.
An
interbody cage with a 10-, 12-, or 14-mm inner diameter packed
with bone chips, derived from the corpectomy, is then placed
for maintaining a original cervical alignment. Intraoperative
radiography
is used to confirm the appropriate placement of the cage before
routine closure of the wound.
Discussion
There are two surgical procedures for the treatment of OPLL: (1) direct removal of the ossified mass via an anterior approach, or (2) decompression in which the techniques of laminectomy or laminoplasty are used, via a posterior approach.[1],[2],[9],[17] Although
the decision should be based on patient age, severity of symptom, type
of OPLL, and the surgeon′s preference, anterior decompression
of OPLL generally achieves more satisfactory results than posterior decompression
in cases of one- or two-level OPLL.[2], [18],[19],[20] However,
CSF leakage occurs during 4.5-32% of multilevel anterior cervical
corpectomies with fusion performed for OPLL.[13],[14] Accumulation of CSF in the wound may cause delay of wound healing, delayed kyphotic deformity, or infection or airway obstruction.[6] Furthermore, nerve root herniation or spinal cord damage may occur through the dural defect during surgical manipulation. Thus, we describe a new technique for avoiding those complications.
DO associated with OPLL has been documented by several authors.[16],[21],[22] It
is almost inherently obvious that CT would be the most accurate method
in such cases. Hida et al. and Mizuno et al. defined the double-layer
sign on CT, which is most coμn in segmental OPLL, as being characterized
by anterior and posterior rims of hyperdense ossification separated by
a central hypodense mass, the hypertrophied but nonossified PLL.[16],[22]
In our technique, the usual necessary discectomies and corpectomies
are performed first to expose the OPLL. OPLL is usually removed using
a high-speed drill with a 4-mm steel burr until it becomes thin, because
the ossified mass is composed of solid lamellar bone. Sporadic bleeding
in OPLL can be managed with packing bone wax. When the OPLL becomes
thin, the head of a drill should be changed from a steel burr to a
diamond burr to prevent accidental damage of the underlying dura mater.
When the OPLL is further thin and cracked, it becomes mobile. At this
point, drilling of the OPLL is terminated, and the thinned-out OPLL
and nonossified hypertrophic PLL are separated from the dura mater,
using a microdissector, and are then resected piecemeal using a 1--2-mm
Kerrison rongeur after a small piece of cotton is inserted into the
space between the OPLL and the dura mater. It could be dangerous to
tilt the residual DO, because of involvement of the dura mater or further
compression of the deformed spinal cord. In fact, minor CSF leakage
occurred during this procedure as shown in Case 3. Therefore, one who
performs this procedure should be careful not to grasp and remove a
large piece of the residual ossified or hypertrophied PLL. This manipulation
prevents the dura mater from tearing due to adhesion. Ossified portion
of the dura mater can be separated from the OPLL, because there is
a thin layer of the PLL between the OPLL and DO in cases of double-layer
pattern. The remaining isolated DO floats and becomes mobile, and eventually
may not compress the spinal cord as shown [Figure - 1].
The indication of this technique is essentially for one- or two-level
segmental OPLL associated with a double-layer DO, while three- or
more-level OPLL is indicated for a posterior approach. Continuous or
mixed-type
OPLL with DO should also treated by a posterior approach, because
the dura mater may be extensively involved in OPLL, and no layer of the
PLL may exist between the OPLL and DO.
References
| 1. | Abe H, Tsuru M, Ito T, Iwasaki Y, Koiwa M. Anterior decompression for ossification of the posterior longitudinal ligament of the cervical spine. J Neurosurg 1981;55:108-16 Back to cited text no. 1 [PUBMED] |
| 2. | Mizuno J, Nakagawa H. Outcome analysis of anterior decompressive surgery and fusion for cervical ossification of the posterior longitudinal ligament: report of 107 cases and review of the literature. Neurosurg Focus 2001;10:6. Back to cited text no. 2 |
| 3. | Nagashima C. Cervical myelopathy due to ossification of the posterior longitudinal ligament. J Neurosurg 1972;37:653-60 Back to cited text no. 3 [PUBMED] |
| 4. | Terayama K, Maruyama S, Miyashita R, Yakubukuro K, Kinoshita M, Shimizu Y, et al. Ossification of the posterior longitudinal ligament in the cervical spine. Orthop Surg 1964;15:1083-95 Back to cited text no. 4 |
| 5. | Tsukimoto H. A case report -autopsy of syndrome of compression of spinal cord owing to ossification within spinal canal of cervical spines. Nippon Geka Hokan 1960;29:1003-7 Back to cited text no. 5 |
| 6. | Chang HS, Kondo S, Mizuno J, Nakagawa H. Airway obstruction caused by cerebrospinal fluid leakage after anterior cervical spine surgery. A report of two cases. J Bone Joint Surg (Am) 2004;86:370-2. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Clements DH, O'leary PF. Anterior cervical discectomy and fusion. Spine 1990;15:1023-5 Back to cited text no. 7 [PUBMED] |
| 8. | Epstein NE. Circumferential surgery for the management of cervical ossification of the posterior longitudinal ligament. J Spinal Disord 1998;11:200-7. Back to cited text no. 8 [PUBMED] |
| 9. | Hirabayashi K, Watanabe K, Wakano K, Suzuki N, Satomi K, Ishii Y. Expansive open-door laminoplasty for cervical spinal stenotic myelopathy. Spine 1983;8:693-9 Back to cited text no. 9 [PUBMED] |
| 10. | Isu T, Kamada K, Kobayashi N, Mabuchi S. The surgical technique of anterior cervical fusion using bone grafts obtained from cervical vertebral bodies. J Neurosurg 1994;80:16-9 Back to cited text no. 10 [PUBMED] |
| 11. | MacDonald RL, Fehlings MG, Tator CH, Lozano A, Fleming JR, Gentili F, et al. Multilevel anterior cervical corpectomy and fibular allograft fusion for cervical myelopathy. J Neurosurg 1997;86:990-7 Back to cited text no. 11 [PUBMED] |
| 12. | Epstein NE, Hollingsworth PA. Anterior cervical micro-dural repair of cerebrospinal fluid fistula after surgery for ossification of the posterior longitudinal ligament. Technical Note. Surg Neurol 1999;52:511-4 Back to cited text no. 12 |
| 13. | Kojima T, Waga S, Kubo Y, Kanamaru K, Shimosaka S, Shimizu T. Anterior cervical vertebrectomy and interbody fusion for multi-level spondylosis and ossification of the posterior longitudinal ligament. Neurosurgery 1989;24:864-72 Back to cited text no. 13 [PUBMED] |
| 14. | Smith MD, Bolesta MJ, Leventhal M, Bohlman HH. Postoperative cerebrospinal fluid fistula associated with erosion of the dura. Findings after anterior resection of ossification of the posterior longitudinal ligament in the cervical spine. J Bone Joint Surg 1992;74:270-7 Back to cited text no. 14 [PUBMED] |
| 15. | Hanai K, Adachi H, Ogasawara H. Axial transverse tomography of the cervical spine narrowed by ossification of the posterior longitudinal ligament. J Bone Joint Surg (Br) 1977;57:481-4 Back to cited text no. 15 |
| 16. | Hida K, Iwasaki Y, Koyanagi I, Abe H. Bone window computed tomography for detection of dural defect associated with cervical ossified posterior longitudinal ligament. Neurol Med Chir (Tokyo) 1997;37:173-6 Back to cited text no. 16 [PUBMED] |
| 17. | Nakagawa H, Mizuno J. The pathophysiology and management of ossification of the posterior longitudinal ligament. In : Barrow DL editor, Perspectives in Neurological Surgery. Quality Medical: St Louis; 1992. p. 38-48 Back to cited text no. 17 |
| 18. | Kirita Y. Posterior decompression for ossification of the posterior longitudinal ligament of the cervical spine. The method of the wide and instantly expansive laminectomy. Orthop Surg 1979;30:45-9 Back to cited text no. 18 |
| 19. | Nakano N, Nakano T, Nakano K. Comparison of the results of laminectomy and open-door laminoplasty for cervical spondylotic myelo-radiculopathy and ossification of the posterior longitudinal ligament. Spine 1988;13:792-4 Back to cited text no. 19 [PUBMED] |
| 20. | Tomita K, Nomura S, Umeda S, Baba H. Cervical laminoplasty to enlarge the spinal canal in multilevel ossification of the posterior longitudinal ligament with myelopathy. Arch Orthop Trauma Surg 1988;107:148-53 Back to cited text no. 20 [PUBMED] |
| 21. | Epatein NE. Identification of ossification of the posterior longitudinal ligament extending through the dura on preoperative computed tomographic examinations of the cervical spine. Spine 2001;26:182-6 Back to cited text no. 21 |
| 22. | Mizuno J, Nakagawa H, Matsuo N, Song JS. Frequency and classification of DO and capability of identification of DO among plain radiographs, polytomography, computed tomography and magnetic resonance imaging in cervical ossification of the posterior longitudinal ligament. J Neurosurg (Spine) 2005;2:425-30 Back to cited text no. 22 |
Copyright 2005 - Neurology India
The following images related to this document are available:
Photo images
[ni05125f3.jpg]
[ni05125f2.jpg]
[ni05125f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}