 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
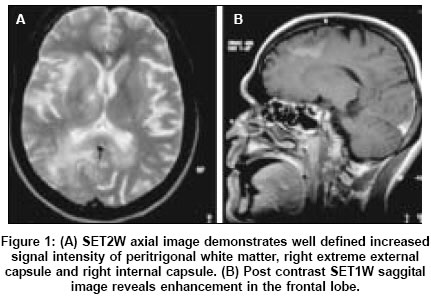
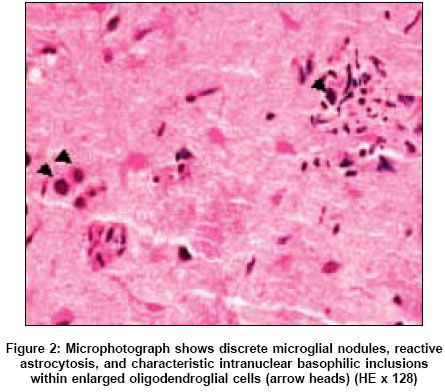
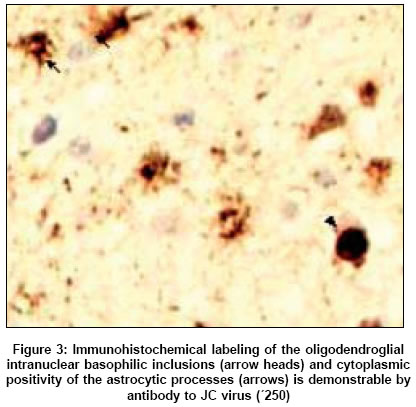
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 358-360 Neurolopathological Discussion A 30-year-old male with diffuse white matter lesions Yasha TC, Anandh B, Srikanth SG, Mahadevan Anita, Santosh Vani, Shankar SK Departments of Neuropathology, National Institute of Mental Health and Neurosciences, Bangalore Date of Acceptance: 17-May-2004 Code Number: ni05126 A 30-year-old male presented with fever and cough with expectoration of 3-month duration. He was diagnosed to have pulmonary tuberculosis and antituberculous therapy was initiated. He developed progressive lower limb weakness over 1 month. He was detected to be HIV seropositive. At the time of admission to the hospital, he was dull, withdrawn, and had spastic paraparesis (Grade 4/5 power). Cerebrospinal fluid (CSF) studies revealed 120 cells/mm3sub, 98% lymphocytes, 62 mg/dl protein. CD4/CD8 counts and HIV viral load could not be done. Serological studies for toxoplasma, Mycobacterium tuberculosis , cysticercal antibodies, and cryptococcal antigen were negative. Chest X-ray was normal. Magnetic resonance imaging (MRI) images (T1, T2, fluid inversion, and contrast enhanced) revealed irregularly enhancing diffuse white matter lesions in the periventricular white matter in right frontal temporal and parietal lobes, extending along the corpus callosum [Figure - 1]A, B. Another small discrete lesion was seen in right thalamus [Figure - 1]. There was no mass effect. To recognize either a treatable infective condition or a neoplastic lesion such as glioma or lymphoma in HIV positive individual, stereotactic biopsy of right frontal white matter lesion was carried out. Microscopic examination Histological examination of the small biopsy tissue revealed dense perivascular lymphocytic infiltrate, multiple discrete microglial nodules at the gray white junction and florid reactive astrocytosis. No glial tumor was noted. Diligent search for toxoplasma, mycobacteria, and fungal bodies was negative. In the midst of the microglial nodules and randomly distributed in the white matter large oligodendroglial nuclei swollen by deeply basophilic inclusions were seen [Figure - 2], arrow. In addition a few small, round calcific concretions were found. Myelin stains revealed myelin pallor. Immunohistochemical staining showed specific and diagnostic labeling of the oligodendroglial intranuclear basophilic inclusions [Figure - 3], arrow and cytoplasmic positivity of the astrocytic processes. Diagnosis Discussion The incidence of PML an opportunistic infection caused by JCV (a polyoma virus) has risen dramatically during the AIDS epidemic. In the West, over 50% of healthy adolescents and adults have serological evidence of primary polyoma viral infection, probably acquired by oral or respiratory route.[1] From India, similar serological data is not available. JCV persists as a latent and asymptomatic infection in B-lymphocytes, kidney, and possibly central nervous system (CNS). Immunosuppressive state with CD4 count <100 cells/mm3sub reactivates the latent infection causing viremia and CNS disease. The characteristic histological features are foci of demyelination rimmed by inclusion bearing oligodendrocytes and bizarre astrocytes of variable morphology. Immunohistochemistry and electron microscopy establishes the diagnosis as in this case where anti-JCV specific antibody labeled the inclusions and the viral antigen in astrocytes. In classical PML, the inflammatory infiltrate is almost exclusively foamy macrophages with sparse lymphocytic reaction. Occasionally however, there is intense inflammation, microglial reaction, and necrosis indicating enhanced immunological response and prognosis. In tropical countries, microglial aggregates in the neuropil and perivascular lymphocytic cuffing denotes viral encephalitis or toxoplasma infection and these need to be investigated for instituting appropriate therapy. In the present era of AIDS, cerebral toxoplasmosis is more coμn in India and takes precedence over PML. The etiology of focal brain lesions in HIV-infection has varied from the pre-HAART (highly active anti retroviral therapy) and HAART eras and commonly includes toxoplasmosis, primary CNS lymphoma (PCNSL), and PML.[2] Mass effect and contrast enhancement favor the former although occasionally PML lesions may also enhance, as in the present case. Based on imaging many neurologists make the diagnosis of PML, yet very few proven cases are reported from India and none from Sub Saharan Africa, though HIV/AIDS are very prevalent. According to recommended consensus terminology, PML cases should be referred to as ′histology - confirmed′ with evidence of JCV infection in brain, ′laboratory - confirmed′ with detection of JCV DNA in CSF or ′possible,′in the presence of typical clinical and radiological picture but no demonstration of JCV infection,[3] to include in clinical trial and to institute appropriate therapy. On MRI, PML typically appears as multifocal scalloping lesions located essentially in white matter, hypointense on T1-weighted image, and hyperintense on T2-weighted images.[4] Increased low signal on T1-weighted image and increased intensity both on FLAIR and T2-weighted images on follow up, either in drug naive HIV positive or HAART-treated PML cases suggests progressive destructive lesion, a poor prognostic sign,[5] as noted in the present case. On the other hand, if the initial progressive disease is halted by HAART treatment, atrophic changes, and leukomalacia in the brain are visualized as increasing low signal on T1-weighted image corresponding low signal on FLAIR images as well representing burnt out process.[6] Development of mass effect and contrast enhancement could represent deranged blood brain barrier either due to rapid progression of the disease or immune activation following HAART therapy. The present case is drug naive and hence contrast enhancement could represent active progression of the disease. In view of these various modulating factors, it is difficult to comment on sensitivity and specificity of MRI in understanding and predicting the biology of PML. MRI lesions progressing in number and volume or both are considered indicative of active PM. On the other hand PML is considered in active, when new lesions are not detected or atrophic changes in old lesions are noted during a maximum interval of 3 months. Paradoxical worsening of MRI lesions may precede radiological improvement or stabilization in patients who are already clinically stable. A polymerase chain reaction (PCR) test on CSF can assist in diagnosis of PML, without resorting to brain biopsy. A number of case-control studies have shown that JCV DNA detection in CSF has a sensitivity of 72-92% and a specificity of 92-100%.[7] However, association of JCV DNA in peripheral blood mononuclear cells may vary considerably among PML patients and viral load is not constant during the course of illness.[8] Current experience suggests that JCV DNA levels fluctuate over time in patients with active PML.[9] Approximately one-third of patients may not have JCV DNA in CSF at the time of PML diagnosis and hence this indicator may not be helpful in assessing the progression of the disease. Histological evaluation of brain tissue obtained by steriotactic biopsy is the standard procedure for etiological diagnosis of PML, in HIV/AIDS related focal lesions. However, it has a sensitivity of 64-94%, sampling error being the most frequent cause for failure to establish definitive diagnosis in clinically suspected cases of PML. On the other hand, the specificity is virtually 100%.[2] It is essential to realize that in inactive PML cases demylinating zones without evidence of viral inclusions and JCV antigen by immunohistochemistry can be seen, even in previously confirmed cases. These lesions can be mistaken for demyelinating lesions caused by healed VZV encephalitis, cerebral malaria, and toxoplasmosis. Significant genetic diversity of JCV has been identified in various geographic regions around the world, with variable permissiveness infecting the glial elements. HIV-1 virus infecting the population of India and Sub Saharan Africa belongs to the subtype C (clade C), while in USA, Europe, Australia, and Japan it is HIV-1 clade B. These two subtypes differ in the genetic constitution of the HIV virus and the transactivating property on coexisting JCV. This may explain the low prevalence of PML in India and Sub Saharan Africa.[10] Some strains of JCV infect glial cells more readily than others. In addition, host factors such as genetic polymorphism in tumor modulating protein P53 may control susceptibility to PML in AIDS and non-AIDS individuals.[11] It has been suggested that the oncogenic potential of JCV could influence the transformation and evolution of gliomas, from the characteristic bizarre ′tumor-like′astrocytes in the PML lesion to overt tumor. However, CNS glial tumors have only rarely occurred in conjunction with PML.[12] HAART has improved the clinical outcome in PML patients with long periods of remission. It acts indirectly by its antiretroviral action, increase CD4 counts, and thereby immunological function. Conversely, patients already on HAART who develop PML within the immune reconstitution period fare poorly.[13] Cidofovir has a beneficial therapeutic response and combined with HAART therapy and has resulted in prolonged survival.[14] Recognition of PML, as a cause of focal brain lesion without mass effect and submitting the CSF for JCV-DNA testing can facilitate rapid diagnosis, provided the test is positive. In the absence of it steriotactic biopsy and demonstration of JC viral antigen by immunohistochemistry remains gold standard. In view of high cost involved and the toxicity of HAART drugs, it may be pragmatic to establish the diagnosis by biopsy, than initiating therapy empirically and altering the course of the disease. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05126f3.jpg] [ni05126f2.jpg] [ni05126f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}