 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
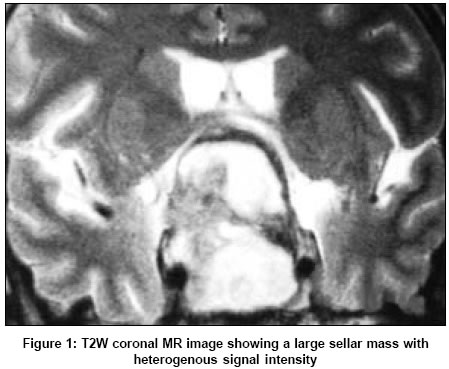
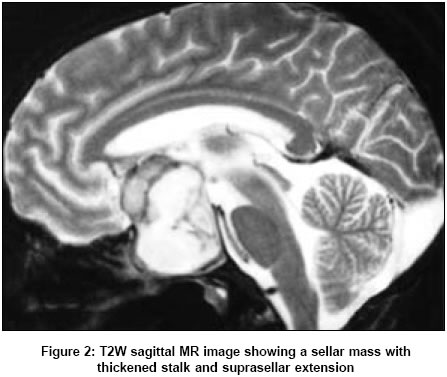
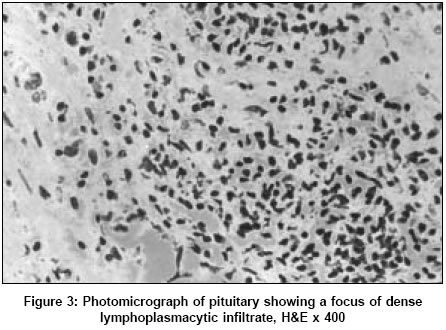
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 363-364 Letter To Editor Lymphocytic hypophysitis presenting as pituitary apoplexy in a male Minakshi B, Alok S, Hillol KP Departments of Pathology and Neurosurgery, Dr. Ram Manohar Lohia Hospital, New Delhi Date of Acceptance: 24-Feb-2005 Code Number: ni05129 Sir, Inflammatory lesions of the pituitary are rare with an estimated incidence of one case in ten million population.[1] Lymphocytic or autoimmune hypophysitis was first described by Goudie and Pickerton[2] in 1962, and since then approximately 379 cases have been reported.[3] Most cases occur in women, mostly during late pregnancy or early postpartum period. Pituitary apoplexy, a clinical syndrome of sudden onset of severe neurological dysfunction due to hemorrhage or infarction of pituitary, usually occurs in the setting of a pre-existing adenoma. Association of pituitary apoplexy and lymphocytic hypophysitis has been reported only twice earlier, both in female patients.[4],[5] A 42-year male presented with progressive deterioration of vision in both eyes over a 1-year period. A contrast enhanced CT scan revealed the presence of a sellar mass suggestive of an adenoma. The patient was advised surgery, but he refused to accept this advice. He was brought in an unconscious state to our institution. A magnetic resonance (MR) image showed a sellar mass with suprasellar extension [Figure - 1], [Figure - 2]. He was treated managed with high-dose intravenous steroids, intravenous fluids, and eltroxine. He progressively regained consciousness within 72 h. Physical examination at this time showed a pale sallow complexion. He was blind in the right eye with temporal hemianopia in the left eye. Visual acuity of left eye was 6/60. Fundus examination showed primary optic atrophy in both eyes. Hormonal profile revealed hyperprolactinemia (4,000 IU/l). The patient also developed polyuria with a urinary volume of 9-12 l/day. He was treated with bromocriptine and prepared for surgery. A right frontal craniotomy using subfrontal approach was performed. Upon incising the diaphragma sellae 5-7 ml of necrotic material was excised. Postoperatively, the patient developed frank diabetes insipidus that needed aqueous vasopressin treatment. His visual acuity did not improve. Haematoxylin and eosin-stained sections from the biopsy showed complete effacement of the pituitary structure by a dense lymphoplasmacytic infiltrate and foci of neutrophilic infiltration, necrosis, and fibrosis [Figure - 3]. No tumor could be identified. Stains for bacteria, fungi, Acid Fast Bacilli and spirochaetes were negative. Immunohistochemistry revealed a polyclonal lymphoid population with a mixture of T and B cells. A diagnosis of lymphocytic hypophysitis was considered. The patient was discharged on a maintenance dose of steroids and is currently on regular follow up. Lymphocytic hypophysitis closely mimics a pituitary adenoma both clinically and radiologically. MR features suggestive of an inflammatory pituitary process include loss of hyperintense bright spot signal of the normal neurohypophysis, thickening of pituitary stalk and enlargement of neurohypophysis in cases where it is involved.[6] A review of literature revealed only two case reports of this association with lymphocytic hypophysitis (both in female patients),[3],[4] and one case with granulomatous hypophysitis (intrasellar tuberculoma).[7] Surgical intervention is required to establish the diagnosis and to reduce the size of the lesion to relieve the mass effect on adjacent structures. Prasad et al.[8] proposed a management paradigm for suspected cases of lymphocytic hypophysitis and advocated a trans sphenoidal stereotactic biopsy to achieve a tissue diagnosis, which might avoid the need for an open exploration of the sella. The present case highlights the fact that apoplectic changes may complicate the course of inflammatory pituitary lesions, thus calling for a greater vigil and clinical judgment in management of these patients. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05129f1.jpg] [ni05129f3.jpg] [ni05129f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}