 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
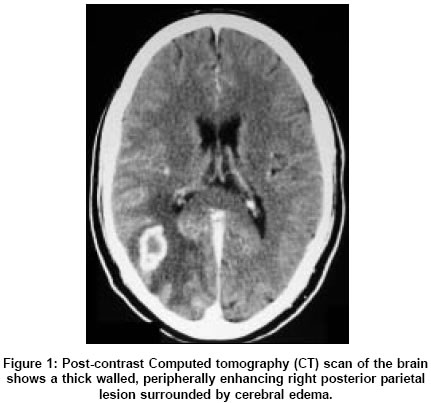
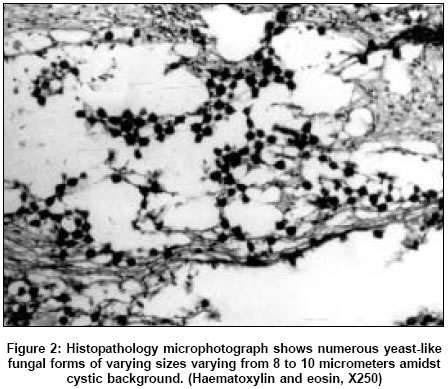
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 365-367 Letter To Editor A solitary cryptococcal granuloma in an immunocompetent host Nadkarni TD, Menon RK, Desai KI, Goel A Department of Neurosurgery, King Edward Memorial Hospital, Seth G. S. Medical College, Parel, Mumbai Date of Acceptance: 10-Mar-2005 Code Number: ni05131 Sir, Cryptococcomas or ′cryptococcal granulomas′ are rare in an immunocompetent host in the absence of cryptococcal meningitis. The morbidity and mortality due to cryptococcosis is high unless it is diagnosed and treated early. A 22-year-old male presented with left focal seizures with secondary generalizations for three years. The patient had no clinical evidence of immunocompromise or meningitis. Human immunodeficiency virus (HIV) antibodies were negative and the CD4 T-cell lymphocyte counts were normal. A computed tomography (CT) scan of the brain revealed a right parietal lesion. It was isodense on plain scan and there was a peripheral enhancement on contrast administration [Figure - 1]. The lesion was surrounded by cerebral edema. The patient was placed on anticonvulsants and on the clinical and radiological suspicion of a tuberculoma the patient was empirically started on anti-tuberculous therapy. The patient was seizure free and had some relief from headaches. After about one year of anti-tuberculous therapy the patient had recurrence of seizures and developed left hemiparesis. CT scan of the brain showed a slight increase in size and of the lesion and surrounding edema. The patient now had bilateral papillodema and left hemiparesis. A stereotactic biopsy of the lesion confirmed that the lesion was a cryptococcal granuloma. The mass was surgically excised. Histopathology showed characteristic features of a fungal granuloma with fibroblasts, giant cells with yeast forms of capsulated fungal elements and necrotic areas. The inflammatory response consisted mainly of lymphocytes, plasma cells, eosinophils, fibroblasts and multinucleated giant cells studded with cryptococci [Figure - 2]. The patient was treated with liposomal amphotericin and anticonvulsants. The patient was seizure free and the left hemiparesis improved. The follow-up is of 9 months. Cryptococci have a strong neurotropic tendency and involve the meninges and brain. Cryptococcosis is an infection caused by yeast like fungus, Cryptococcus neoformans.[6] The infection occurs due to inhalation of fungus into the lungs. Hematogenous spread to the brain leads to clusters of cryptococci in the periventricular areas of cortical grey matter and basal ganglia. The leptomeninges become infiltrated, thickened and opaque. The Virchow-Robin spaces around penetrating vessels are distended with organisms; most of the patients have co-existent meningitis. Granulomatous lesions may be found in the cerebral or spinal parenchyma. In our patient a cryptococcal granuloma was identified in the parietal parenchyma in the absence of meningitis. There are few, isolated reports of cryptococcal infection in immunocompetent patients in literature. [1],[2],[3],[4] Such previously reported cases include a cryptococcoma in the pituitary,[1] pons,[2] crytococcal meningitis [3], midbrain [4], and cerebellum.[5] Data suggest an association between cryptococcal variety and host immune status.[6] The varieties of Cryptococcus neoformans serotypes are neoformans and gattii. These two varieties differ in their epidemiology and pathogenicity. Furthermore, symptoms, outcome, and response of cryptococcosis to antifungal therapy may vary. The two varieties also differ in immune-modulating effects. Sparse clinical data suggest the gattii variant to be more virulent and more recalcitrant to antifungal therapy. A better understanding of how cryptococcal variety influences the clinical course and response to the treatment of cryptococcosis is needed. Clinicians should be aware of the association, especially in patients with refractory disease. It may be useful to type the isolate to the variety level and administer prolonged antifungal therapy. Early aggressive therapy has the best chances of cure. All the above patients including ours have been treated with Amphotericin B. Presently liposomal amphotericin ameliorates the adverse effects of plain amphotericin and ensures better brain penetration of the drug. Flucytosine or miconozole are alternative drugs. Surgical excision with concomitant medical therapy offers the best results. Image based diagnosis of intracranial tuberculoma is fairly accurate in patients from endemic regions and it is not considered necessary to obtain a histological diagnosis. However, Selvapandian et al[7] have demonstrated the low positive predictive value for a diagnosis of intracranial tuberculoma on CT alone and they stress the need for confirming histological diagnosis. Surgical excision is feasible when such a lesion is easily accessible and not in an eloquent area. In conclusion, the possibility of a fungal granuloma needs to be considered in an indolent lesion in an immunocompetent host. Histological diagnosis before initiating empirical therapy is recommended for all intracranial masses. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05131f2.jpg] [ni05131f1.jpg] |
| |||||||||

{kind=link}
{kind=link}