 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 367-368 Letter To Editor Distress triggered cervical root compression pain by looped vertebral artery Kalkan E, Paksoy Y, Reisli R, Topatan Hi Departments of Neurosurgery, Selcuk University, Meram
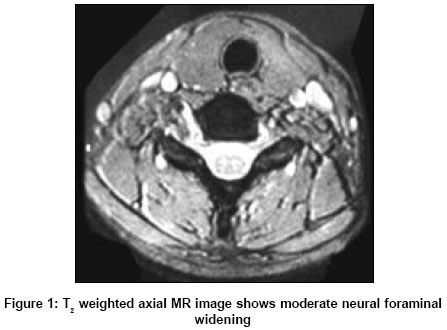
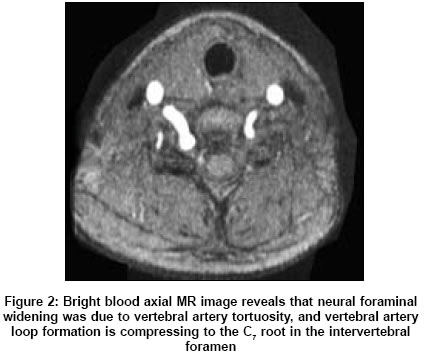
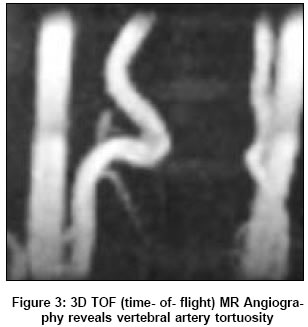
Medicine Faculty, Konya Date of Acceptance: 04-Apr-2005 Code Number: ni05132 Sir, A 21-year-old girl presented with a 20-day history of right-sided cervicobrachialgia radiating in her hand and fingers. Whenever she was distressed, she experienced the pain associated with involuntary movements and the absence of nocturnal recrudescence and hypoesthesia of right thumb. History of familial neurofibromatosis and cervical spine trauma were absent. Both the physical and neurological examination was normal. However neither vascular bruit nor pain compliance has been detected. Cervical right oblique X-ray showed a minimal and T2 weighted axial MRI showed moderate foraminal widening at C6 - 7 intervertebral foramen [Figure - 1]. Bright blood axial MR images revealed that vertebral artery loop compressed the C7 root in the intervertebral foramen [Figure - 2]. The 3D TOF (time-of-flight) MR Angiography showed a vertebral artery tortuosity [Figure - 3]. The patient refused an operation against further disturbances. Tricyclic anti-depressant Amitriptyline was given 10 mg for first 3 days, and continued 20 mg at night. All symptoms relieved and analgesia achieved within 2 days. Progressive cervical radiculopathy due to loops of the vertebral artery is seen rare. The average age was 55 and our case is the youngest one as compared with in previous reports. However, the mechanism of how VA loop forms is unclear. A cervical trauma and spondylotic changes with the degree of VA tortuosity has been reported.[1],[2],[3],[4] But our case has neither spondylosis nor cervical trauma. It is difficult to distinguish the tortuosity of the vertebral artery from expected clinical symptoms with cervical myelopathy or radiculopathy in patients. It is emphasized that the frequent acroparesthesia and dysesthesia of fingers, and rare neurological deficits and nocturnal recrudescence are quite valuable in differential diagnosis.[5] We suggest that the anxiety because of stress-elevated intra-arterial blood pressure triggers the radiating pain in our case. An axial MR is a valuable scan as evaluation of loop formation. If MRI findings suggest any possible VA tortuosity and migration, then MR angiography should be performed to confirm these findings.[3] In treatment modalities, it has been experienced that most patients require surgical procedures in spite of they were treated conservatively initially. The traditional surgical procedures are anterolateral microvascular decompression and anterolateral cervical vascular reconstruction of the loop vertebral artery.[5] Mild sedatives relieved symptoms. Surgery has been advised as preventive for further progressive disturbances. However she refused the surgical procedure. The onset of analgesia with tricyclic anti-depressants ranges from 3 to 7 days for radicular pain. Pain relief in this patient showed us that within 2 days sedation (one of coμn side effects of amitriptyline) was effective to relieve the stress of patients as well as the stress related to hypertension. In our further investigations, we saw that she was calm, and her blood pressures were at normal levels. This case is, the youngest and only case with a pain aggravated by anxiety as far as we have seen in vertebral artery compression syndromes. Loop compression has some characteristics, which differentiate it from other cervicobrachialgia syndromes. The MR with MR angiography is the preferred modality in diagnostic work-up. Conventional angiography may be indicated only if the vascular reconstruction is planned for the compressive evaluation, which includes the balloon occlusion test. Acknowledgments I would like to thank Associate Professor M. Erkan Ustun and Assistant Professor Ali Gunes for their invaluable help during the process of writing this article.References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05132f1.jpg] [ni05132f2.jpg] [ni05132f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}