 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 368-370 Letter To Editor Intracranial actinomadura granuloma Sujit Kumar GSamson, Chacko Geeta, Mathews MaryS, Mathew JohnM Section of Neuropathology, Department of Neurological
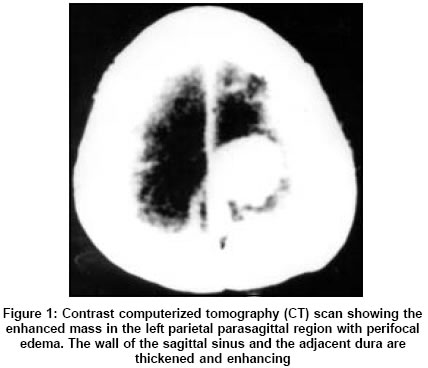
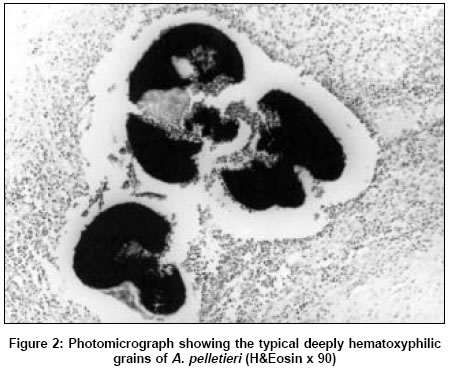
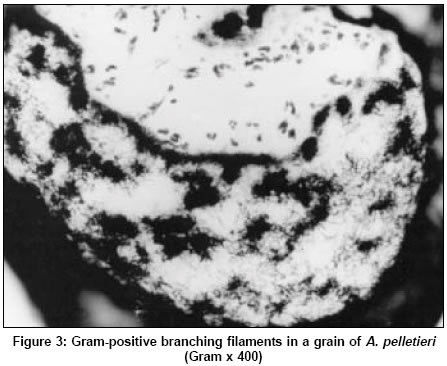
Sciences, Christian Medical College and Hospital, Vellore - 632 004 Date of Acceptance: 10-Apr-2005 Code Number: ni05133 Sir, Intracranial granulomas caused by aerobic bacteria of the actinomycetes group are rare. We report a case of an intracranial granuloma caused by Actinomadura pelletieri . Our literature survey did not reveal any report of such a granuloma. A 24-year-old woman presented with headache of 1-year and seizures of 1-month duration. About a week prior to the onset of the seizures, she had developed a swelling on the scalp close to the midline in the left parietal region discharging pus intermittently. She had history of injury to the scalp, ten years earlier. An excision was done elsewhere, the biopsy was not sent and routine cultures were negative. The wound did not heal primarily and despite antibiotics she developed a persisting discharging sinus at the site of the incision. Plain X-ray skull showed evidence of osteomyelitis and computerized tomogram (CT) of the head revealed a hyperdense, contrast enhancing lesion in the left parietal parasagittal region, with significant perifocal edema. The sagittal sinus and adjacent dura were thickened and enhancing [Figure - 1]. Clinically she had bilateral papilloedema and right lower limb weakness. At surgery, there was large collection of pus and infected granulation tissue between the fascial planes of the scalp. The bone was osteomyelitic and the dura was thickened and adherent to the underlying lesion. The lesion was firm, grayish white and avascular with reddish granules on the surface. On histology there were multiple microabscesses within which were granules [Figure - 2]. Gram stain showed slender irregularly stained gram-positive filaments [Figure - 3]. Two weeks later, the cultures on saboraouds dextrose agar (SDA) grew colonies, which were heaped, glabrous, cerebriform, and coral red in color with no aerial mycelium or diffusible pigment which is typical of this organism. The identification of the organism as Actinomadura pelletieri was confirmed by Centers for Disease Control and Prevention, Atlanta, GA 30333, USA (Lab. No. 97019255). She was started on high dose of cotrimoxazole (trimethoprim and sulphamethoxazole). Postoperatively the wound healed primarily. The seizures were well controlled with medication and the weakness in the leg gradually improved to normal. Actinomadura pelletieri are aerobic, nonfastidious gram-positive branching organisms. Optimum temperature for growth is 37°C, which is usually slow and takes about 2-3 weeks for the colonies to appear. The colonies are dry, adherent, waxy, and have a characteristic coral red nondiffusible pigment. There are a few reports of this organism causing mycetoma both of the foot and extrapedal locations including the scalp. [1],[2],[3] This organism gets inoculated into the skin through minor injuries and over a period of time, under appropriate conditions causes a chronic suppurative infection. The infection spreads along subcutaneous fascial planes and forms numerous small abscesses, which drain via multiple sinus tract, discharging coral red granules. There is no cementing substance produced by this organism, which probably contributes to its rapid contiguous spread.[4] The haemotoxylin and eosin (H&E) stained sections show abscess cavities containing typical grains which are about 0.3-0.5 mm in diameter, often semilunate and deeply stained by hemotoxylin. These, unlike the grains of Actinomadura madurae, have a sharply delineated border without the fringe of hyphal tips. They are so typical that a specific diagnosis of A. pelletieri can be made with considerable certainty by low power examination of the H&E stain. In this patient, the organism may have got implanted subcutaneous, at the time of the scalp injury. The discharging sinus and the symptoms of intracranial involvement appeared simultaneously indicating a more recent onset of growth after lying dormant for many years. Since the entire lesion was localized to one area, the lesion seems likely to have spread contiguously rather than by a hematogenous spread. At surgery, total excision was carried out as this offers the best chance of cure and postoperatively she was put on cotrimoxazole to which the organism is sensitive.[5] This case, re-emphasizes the need to consider a fungal like infection caused by bacteria of the actinomycetes group, apart from tuberculosis in any intracranial mass with infection in different planes and an overlying discharging sinus. Appropriate cultures and stains would then be required to reveal the true nature of the organism and ensure that appropriate therapy is instituted. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05133f2.jpg] [ni05133f1.jpg] [ni05133f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}