 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
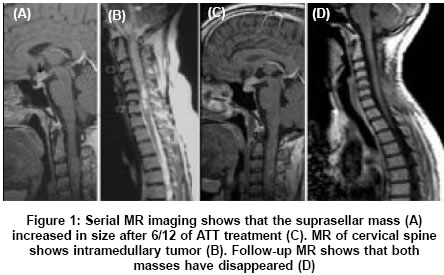
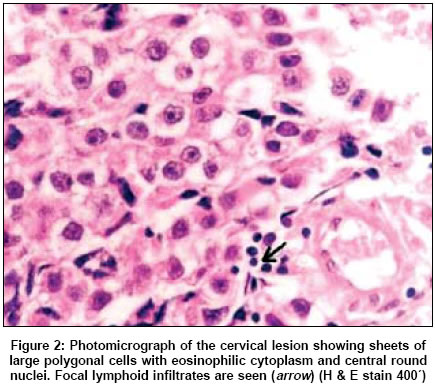
Neurology India, Vol. 53, No. 3, July-September, 2005, pp. 374-375 Letter To Editor Spinal intramedullary metastasis from intracranial germinoma Shah KC, Chacko Geeta, John Subhashini, Chacko AriG Department of Neurological Sciences, and Radiation Therapy, Christian Medical College, Vellore, Tamilnadu Date of Acceptance: 29-Aug-2005 Code Number: ni05138 Sir, Germinomas in the central nervous system (CNS) usually occur in the pineal or the suprasellar regions; less frequent sites include the thalamus, basal ganglia and cerebellar vermis. Metastases to the spine from brain tumors, ′drop metastases′, are usually intradural extramedullary masses. However, they rarely present as intramedullary tumors.[1] A 30-year-old female with amenorrhoea for 1.5 years and galactorrhoea for 6 months had a magnetic resonance image (MRI) of the brain that showed an 8 mm enhancing lesion in the pituitary stalk and hypothalamus [Figure - 1]A. Her hormonal tests were suggestive of panhypopituitarism and she was given thyroid and steroid replacements. The possibilities of a hypothalamic hamartoma or granuloma were considered. She had been started on antituberculous therapy (ATT) elsewhere. After a discussion with the patient and family regarding the risks and benefits of surgery in obtaining a diagnosis, it was decided to follow her up with a repeat image after 6 months and the ATT was continued. Six months later, she had paraesthesiae in both upper limbs, progressive weakness in all four limbs and difficulty in walking. Her gait was spastic but she could walk unaided. An MRI of the cervical spine and brain showed an intramedullary lesion from C1 to C6 levels [Figure - 1]B and slight increase in the size of suprasellar lesion. Cerebrospinal fluid (CSF) analysis showed a total count of 18/cumm, protein 47 mg%, and sugar 55 mg%. CSF beta-hCG was 67 mIU/ml (normal levels 0.0-5.0 mIU/ml) and alpha-fetoprotein was <2 mIU/ml (normal level 0.0-5.5 mIU/ml). She underwent a C1-C7 laminectomy and subtotal excision of the intramedullary tumor. At surgery, there was an exophytic component of the tumor at C2 level and there were areas of necrosis and haemorrhage with a poor tumor-cord interface. Microscopic examination revealed sheets and alveolar clusters of large polygonal cells with abundant eosinophilic to clear cytoplasm and central, round mitotically active nuclei containing prominent eosinophilic nucleoli [Figure - 2]. Immunohistochemical staining was positive for placental alkaline phosphatase and negative for cytokeratin, S100 protein and CD30. A histological diagnosis of a germinoma was made. She underwent three cycles of combination chemotherapy with ′cisplatin′, etoposide and bleomycin followed by craniospinal irradiation (Cobalt 60). A total dose of 36 Gy in 18 fractions was delivered using two parallel opposing fields for the cranium and direct posterior field for the spine. In addition 14 Gy in seven fractions was given as a boost to the cranial and spinal lesion. Contrast enhanced cranial and spinal MRI, 9 months postoperative, showed complete resolution of cranial and spinal lesion [Figure - 1]D. Germinomas constitute 0.1-3.4% of all intracranial tumors with the highest incidence of 4-19% in Japan.[2] The majority of germinomas in the CNS arise extraaxially from the pineal or suprasellar regions . Spinal cord intramedullary germinomas are rare, most having been described in young Japanese adults. [3],[4],[5],[6] In 1985, Hisa et al. were the first to report a case of an intramedullary spinal cord germinoma in a young male patient who had manifested with precocious puberty.[3] Subsequently, a few other reports of intraspinal germinoma have been reported in the literature. [4],[5],[6] Radiation therapy is the treatment recommended for germinomas and most tumors respond well.[7] However, prophylactic irradiation of the entire neuraxis is controversial, and Shibamoto et al. have concluded that the risk of a spinal metastasis from an intracranial germinoma is too low to warrant routine prophylactic spinal irradiation.[1],[7] Sole usage of radiation requires a dose of 40-55 Gy which can cause endocrine disorders and neurocognitive impairment. The risk of these side effects may be reduced by lowering the dose and field size of radiation for young patients, since and late sequelae in survivors have been of major concern. To minimize the post-treatment adverse effects many centers now use induction chemotherapy followed by radiotherapy. Cisplatin-based chemotherapy has proved to be effective for the treatment of intracranial germ cell tumors. For pure germinomas, induction chemotherapy followed by whole brain radiotherapy up to 24 Gy has been shown to be very effective.[8] We elected to treat our patient with induction chemotherapy and craniospinal radiation therapy. Our patient remains in complete remission, but needs close long-term follow up. References
Copyright 2005 - Neurology India The following images related to this document are available:Photo images[ni05138f2.jpg] [ni05138f1.jpg] |
| |||||||||

{kind=link}
{kind=link}